

Abstract
Despite treatment guidelines recommending observation for men with low‐risk prostate cancer with life expectancy <10 years, a majority of elderly patients choose active treatment, which may result in overtreatment. Given the growing burden of prostate cancer among men aged ≥80 years (super‐elderly men), accumulation of survival data for evaluation of overtreatment among super‐elderly patients is imperative. Here, we report results of a population‐based cohort study to clarify potential overtreatment of super‐elderly men with localized prostate cancer. We used cancer registry data from the Monitoring of Cancer Incidence in Japan project, which covers 47% of the Japanese population. The subjects were men diagnosed with prostate cancer between 2006 and 2008. Follow‐up period was 5 years. We calculated 5‐year relative survival rates among the active treatment and observation groups after imputation for missing values. Of the 48 782 patients with prostate cancer included in the analysis, 15.1% were super‐elderly men. The 5‐year relative survival rates of super‐elderly men with localized cancer were 105.9% and 104.1% among the active treatment and observation groups, respectively. This excellent relative survival rate in the observation group remained consistent even after stratification by tumor grade. Of the 2963 super‐elderly men with localized cancer, 252 (8.5%) with curative treatment and 1476 (49.8%) with hormone therapy were assumed to have been overtreated. The proportion of overtreatment was estimated to reach 80% after imputation. These specific survival data in super‐elderly men in the observation group can be useful in shared decision‐making for these patients and may lead to a reduction in overtreatment.
Keywords: 80 years and older, Japan, localized prostate cancer, overtreatment, relative survival
Prostate cancer is the most frequently diagnosed cancer among men in developed countries.1 As life expectancy has lengthened, the incidence of prostate cancer has increased among elderly men.2 From 2015 to 2050, the number of people aged ≥80 years (so‐called super‐elderly people3) is estimated to increase 3.5‐fold worldwide,4 leading to a growing burden of prostate cancer among super‐elderly men.
The prevalence of PSA testing has resulted in a shift to diagnosis of early‐stage prostate cancer.2, 5 Taking account of the higher competing risk of mortality with increased age, quite a few super‐elderly men with low‐risk prostate cancer are expected to be more likely to die of other causes than prostate cancer.6 For such patients, observation may be a reasonable choice because unnecessary treatment (overtreatment) increases medical costs and the incidence of adverse effects, such as urinary, erectile, and bowel toxicity.7 Thus, many urologists have expressed strong concern about identifying those patients who are more likely to obtain benefit from observation. However, considerable variation in the use of observation for men with low‐risk prostate cancer has been seen at the urologist and clinical practice levels, in part due to insufficient evidence to help guide treatment decisions.8, 9
Several population‐based observational studies and a few randomized controlled trials have failed to show a survival benefit for active treatment for men with low‐risk prostate cancer, including surgery,10, 11, 12 radiation,12, 13, 14 and hormone therapy,15, 16, 17 compared with the observation group over 10 years of follow‐up. Based on these findings, treatment guidelines recommend observation for men with low‐risk prostate cancer with life expectancy of less than 10 years.18, 19 Nevertheless, only 20–35% of elderly men with low‐risk prostate cancer actually choose observation as initial therapy.8, 20, 21 The choice of active treatment by a majority of elderly patients may be due to the lack of consistent findings from high‐quality randomized controlled trials.22 What is more, we believe that the tendency to choose active treatment also results from a lack of specific survival data in elderly patients with or without treatment.
Most of the earlier studies mentioned above excluded super‐elderly men10, 11, 12, 20 or reported only one outcome measure for the whole age group.14, 15, 16, 17 Thus, it seems unclear whether these survival data are applicable to the subgroup of super‐elderly patients, who have a larger competing risk of mortality than younger men. Specific survival data of super‐elderly patients are useful for both urologists and patients to decide whether active treatment or observation should be selected. Furthermore, shared decision‐making based on such specific data may lead to reduced overtreatment among super‐elderly men with low‐risk prostate cancer.
Here, we analyzed data from a large population‐based cancer registry in Japan to describe clinical characteristics and survival outcomes among super‐elderly men with prostate cancer. The main aim of this cohort study was to clarify potential overtreatment among super‐elderly men diagnosed with localized prostate cancer.
Materials and Methods
Study group
Patients with prostate cancer were identified from the database of the Monitoring of Cancer Incidence in Japan project. The data were collected from several population‐based cancer registries in Japan. Details of the framework have been described elsewhere.23 The data used in the present study were originally intended to be used in calculating the 5‐year relative survival of patients diagnosed with cancer during 2006 and 2008 in 27 of 47 prefectures in Japan. Follow‐up of each patient was accordingly limited to just 5 years or until death, whichever occurred first. Of the 27 prefectures, 6 were excluded because the information accuracy of their cancer registries did not meet the criteria considered to indicate “high quality”,23 namely: (i) DCO% (proportion of cases reported by death certificate only) <25%, or DCN% (proportion of patients first notified by death certificate) <30%; (ii) M/I <0.67; and (iii) proportion of patients with unknown 5‐year prognosis on overall survival <5%. The overall DCO% and M/I were 13.4% and 0.46, respectively.23 The cancer registries in the remaining 21 prefectures cover approximately 47% of the Japanese population, and include both metropolitan and rural areas (Fig. S1). We identified International Classification of Diseases for Oncology (third edition) code C61.9 as prostate cancer cases. Patients diagnosed with secondary cancers, reported by DCO, or aged ≥100 years were excluded. Finally, 48 782 men with prostate cancer were included.
Variables
Age at diagnosis was categorized into <75, 75–79, and ≥80 years. The group aged 75–79 years was separately categorized to divide men under 80 years old into men with or without approximately 10 years’ life expectancy (<75 years or 75–79 years). Stage at diagnosis was classified into localized (cancer is confined to prostate), regional (cancer spreads beyond prostate into surrounding tissues or regional lymph nodes), or distant (cancer has distant metastases) according to the SEER staging system.24 Tumor grade was classified into well, moderately, and poorly differentiated according to the WHO's classification. If the Gleason score was provided by the medical institution, but degree of tumor differentiation was not, it was classified based on the Gleason score by registry staff at data entry in each cancer registry. Well, moderately, and poorly differentiated corresponds to Gleason scores of 2–4, 5–6, and 7–10, respectively. Because the Gleason score was not required information in Japanese population‐based cancer registries, no information on original Gleason scores could be identified. We excluded undifferentiated carcinoma due to its scarcity (n = 65). We recorded sequential treatment (surgery, radiation, and hormone therapy) started within approximately 4 months after prostate cancer diagnosis. Regarding surgery or radiation, only treatment with curative intent was recorded as sequential therapy. Information on specific surgical procedures, dose of radiation, and the sequence of each therapy was unavailable; for example, neoadjuvant hormone therapy with radiation therapy could not be identified. Initial treatment types for localized prostate cancer were categorized into the following groups: surgery group, those who underwent surgery with or without the other therapies; radiation therapy group, those who underwent radiation therapy with or without additional hormone therapy; and hormone therapy group, those who received only hormone therapy (medication or orchiectomy). In addition, patients in the surgery or radiation therapy group were incorporated into the curative treatment group because few men aged ≥80 years underwent curative surgery. Those who underwent none of the above therapies were defined as the observation (non‐treatment) group.
Statistical analysis
The cancer registry included data on overall survival regarding prognosis. We therefore estimated 5‐year relative survival rates using the Ederer II method (strs command in Stata software; [StataCorp, College Station, TX, USA]) to adjust competing causes of death in patients with prostate cancer.25 Relative survival was the ratio of the observed survival (overall survival) and the expected survival in the cancer‐free general population of the same age, reflecting survival of patients compared to survival of the general population. We used the Japanese general population life tables to estimate expected survival.26 The relative survival has been preferably used to estimate survival in a population‐based setting because it can directly or indirectly capture mortality related to the cancer without requiring information on cause of death.27 An estimation of the 5‐year relative survival of 100% suggests that the survival of the patients is as good as that in the general population, indicating that the patients have not experienced any excess mortality associated with prostate cancer during the first 5 years of follow‐up. If the relative survival rate for untreated patients was above 100%, we assumed patients with active treatment in the same category of tumor stage and grade as the “overtreatment” group. Three categorical variables, tumor stage, grade, and treatment, were incomplete. We therefore applied the method of multiple imputation by chained equation to handle missing values.28 This imputation procedure included survival time itself. We created and separately analyzed 10 imputed datasets, and then combined estimates of relative survival rates and standard errors using Rubin's rule.29 All analyses were undertaken using Stata statistical software version 13.1.
Results
Of 48 782 men, 7370 (15.1%) were aged 80 years and older. The proportion of localized, regional, and distant cancer among men aged ≥80 years was 40.2%, 13.4%, and 17.5%, respectively (Table 1). These proportions after imputation were 58.4%, 18.1%, and 23.5%, respectively. The proportion of localized cancer decreased with increasing age. In contrast, the proportion of distant cancer increased with increasing age. Proportions in the observation group ranged from 11% to 14% across age categories, and men ≥75 years of age were more likely to be untreated. After imputation, the proportion of untreated men was 18.9% among patients aged ≥80 years. The proportion of well to moderately differentiated cancer decreased with increasing age, whereas that of poorly differentiated cancer increased with increasing age. The number of super‐elderly patients with or without active treatment is shown by tumor stage and grade in Table S1.
Table 1.
Clinical and pathological characteristics of patients with prostate cancer according to age categories (n = 48 782)
| Before imputation | After imputation | |||||
|---|---|---|---|---|---|---|
| Age category, years | Age category, years | |||||
| <75 (n = 31 195) | 75–79 (n = 10 217) | 80+ (n = 7370) | <75 | 75–79 | 80+ | |
| Age, years, mean ± SD | 66.9 ± 5.5 | 76.8 ± 1.4 | 83.5 ± 3.4 | |||
| Stage, n (%) | ||||||
| Localized | 17 641 (56.6) | 5163 (50.5) | 2963 (40.2) | (71.5) | (68.6) | (58.4) |
| Regional | 4557 (14.6) | 1262 (12.4) | 990 (13.4) | (18.0) | (16.5) | (18.1) |
| Distant | 2596 (8.3) | 1131 (11.1) | 1290 (17.5) | (10.5) | (14.9) | (23.5) |
| Unknown | 6401 (20.5) | 2661 (26.0) | 2127 (28.9) | |||
| Treatment, n (%) | ||||||
| Active treatment | 21 738 (69.7) | 6302 (61.7) | 4441 (60.3) | (86.2) | (81.6) | (81.1) |
| Observation | 3430 (11.0) | 1445 (14.1) | 1022 (13.9) | (13.8) | (18.4) | (18.9) |
| Unknown | 6027 (19.3) | 2470 (24.2) | 1907 (25.9) | |||
| Grade, n (%) | ||||||
| Well | 5472 (17.5) | 1504 (14.7) | 667 (9.1) | (24.0) | (20.9) | (15.1) |
| Moderately | 10 081 (32.3) | 2990 (29.3) | 1800 (24.4) | (43.6) | (42.2) | (39.6) |
| Poorly | 7374 (23.6) | 2549 (25.0) | 2004 (27.2) | (32.4) | (36.9) | (45.4) |
| Unknown | 8268 (26.5) | 3174 (31.1) | 2899 (39.3) | |||
Table 2 shows the proportions of initial treatment for localized cancer across age categories. Curative treatment (surgery plus radiation therapy) was more frequent among patients aged <75 years. The proportion of patients who received hormone therapy increased with increasing age, and approximately half of patients 80 years and older received hormone therapy. After imputation, of patients 80 years and older, 80.1% received active treatment.
Table 2.
Initial treatment in patients with localized prostate cancer (n = 25 767)
| Before imputation | After imputation | |||||
|---|---|---|---|---|---|---|
| Age category, years | Age category, years | |||||
| n (%) | <75 | 75–79 | 80+ | <75 | 75–79 | 80+ |
| Active treatment | ||||||
| Curative treatment (surgery + radiation) | 10 473 (59.4) | 1261 (24.4) | 252 (8.5) | (70.9) | (34.2) | (14.9) |
| Hormone therapy | 2264 (12.8) | 1996 (38.7) | 1476 (49.8) | (16.5) | (48.8) | (65.2) |
| Observation | 1630 (9.2) | 539 (10.4) | 368 (12.4) | (12.7) | (17.1) | (19.9) |
| Unknown | 3274 (18.6) | 1367 (26.5) | 867 (29.3) | |||
Figure 1 shows relative survival stratified by tumor stage (localized, regional, and distant). For regional and distant cancer, relative survival rates tended to decrease with increasing age and years after diagnosis. Among men aged ≥80 years, 5‐year relative survival rates of regional and distant cancer were 90.7% and 50.4%, respectively. In contrast, for localized cancer, patients in all age categories had 5‐year relative survival rates above 100%. In addition, both the active treatment and observation groups had relative survival rates among men with localized cancer over 100% in all age categories (Fig. 2). The 5‐year relative survival rates of super‐elderly men with localized cancer were 105.9% and 104.1% among the active treatment and observation groups, respectively.
Figure 1.
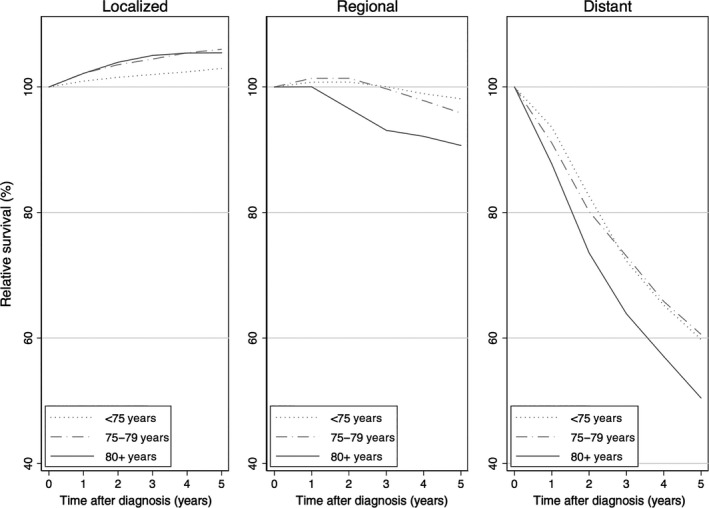
Relative survival of patients with prostate cancer by tumor stage.
Figure 2.
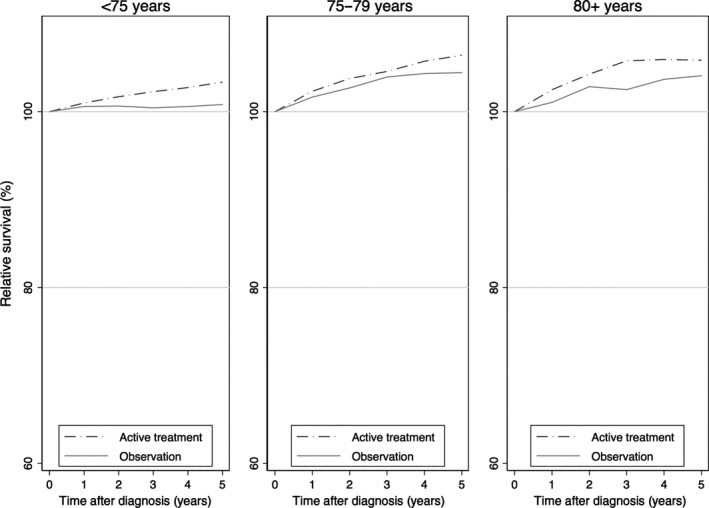
Relative survival of patients with localized prostate cancer with or without active treatment.
To better evaluate the groups of patients receiving overtreatment, we estimated relative survival among untreated men with localized cancer stratified by tumor grade (Fig. 3). For well and moderately differentiated localized cancer, 5‐year relative survival rates were over 100% in all age categories. For poorly differentiated localized cancer, the 5‐year relative survival rate was near or above 100% among men aged ≥75 years, whereas men aged <75 years had a slightly lower 5‐year relative survival rate without active treatment, albeit without statistical significance. The 5‐year relative survival rates and 95% confidence intervals in Figures 1, 2, 3 are shown in Table S2. Furthermore, when stratified by initial treatment type (curative treatment or hormone therapy), no statistically significant decrease in relative survival rate was observed among men aged ≥80 years (Fig. S2). As expected, among treated men with localized cancer, 5‐year relative survival rates were over 100% irrespective of tumor grade (Fig. S3). Based on the results, of 2963 men aged ≥80 years with localized cancer, 252 (8.5%) with curative treatment and 1476 (49.8%) with hormone therapy were assumed to have been overtreated.
Figure 3.
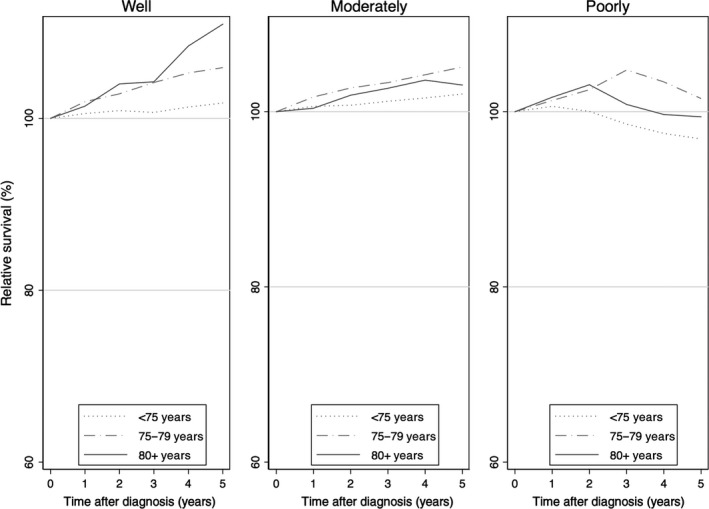
Relative survival of untreated patients with localized prostate cancer stratified by tumor grade.
Discussion
In this study, we describe the clinical and pathological characteristics of super‐elderly men with prostate cancer and relative survival stratified by tumor stage and grade. Our findings indicate that super‐elderly men with localized prostate cancer could live as long as the general population of the same age regardless of tumor grade, even if they received no active treatment.
The overall high relative survival among men with localized cancer may reflect the fact that early‐stage prostate cancer is more likely to be detected by PSA screening.5 Men who receive PSA screening may be more health‐conscious than those in general, given that healthier patients tend to receive preventive therapy (so called “healthy user bias”).30 Thus, men with localized cancer may have better survival outcomes than those of the same age in the general population.
Our findings indicate that at least 58.3% of super‐elderly men with localized prostate cancer were potentially overtreated. After imputation of missing values, this proportion was estimated to reach 80%. Similar high proportions of overtreatment have been reported in the USA.7, 31, 32 Using the SEER data from 2000 to 2002, Miller et al.31 estimated that 55% of men with low‐risk prostate cancer were overtreated. In that study, 42% of men aged ≥75 years were estimated to be overtreated. In a similar way, Aizer et al.7 used data from the SEER‐Medicare Program between 2004 and 2007 and estimated that 67% of men with a life expectancy of less than 10 years were overtreated. These previous studies in the USA had several methodological differences from our study, including category of cancer risk, age range of subjects, and definition of overtreatment. Thus, it is difficult to compare the proportion of overtreatment with that of our study. However, the relatively higher proportion of overtreatment in Japan might be due to differences in clinical practice, and patient and urologist preferences. A universal health insurance system in Japan may also be partly responsible for overtreatment. The small economic burden of health care costs for patients may result in overuse of medical service.33
Previous studies have reported the excellent long‐term survival outcome of men with localized prostate cancer among the observation group.10, 11, 12, 13, 14, 15, 16, 17 However, it has remained unknown whether long‐term survival data among younger patients are applicable to super‐elderly patients, because super‐elderly men with prostate cancer are more likely to die of other causes than cancer within 10 years.6 For example, Wong et al.20 showed that active treatment for even low‐risk localized prostate cancer was associated with a survival advantage among men 65–80 years old. Their important information indicated that there was a long‐term (12 years) survival benefit to active treatment for localized cancer among younger patients. This finding seems inconsistent with our finding that there was no survival benefit for super‐elderly men with localized cancer regardless of tumor grade. This may be because the previous study excluded super‐elderly men and focused on long‐term survival outcomes. We agree with the importance of studies that examine survival outcomes among a wide range of age groups as a source of general information. However, we would like to emphasize the importance of setting an appropriate follow‐up period that is consistent with the life expectancy of the subjects of interest. Specific survival data may be more applicable to patients among particular age groups.
Due to the long natural history of localized prostate cancer, observation is considered an effective means of decreasing overtreatment.18 However, a majority of super‐elderly men with localized cancer received active treatment. Previous studies have suggested that several barriers prevent super‐elderly men from selecting observation as initial therapy. One barrier is patient anxiety regarding not treating the cancer.34, 35 Even with awareness of the possibility of significant adverse effects, patients with low‐risk cancer tend to receive active treatment due to the fear of cancer progression.34 Another barrier is insufficient support and information offered by physicians.34, 36 Davison et al.36 found that men aged >70 years preferred to play a passive role in treatment decision making, and some studies concluded that physician recommendations in the choice of treatment are the most important factor in the patients’ decision to select active surveillance.36, 37 Gorin et al.37 reported that only 36% of patients with low‐risk prostate cancer were provided with an active surveillance option by physicians. Furthermore, Mitsuzuka et al.38 found that active surveillance was not used among a large sample of 26.9% of urologists in Japan. They showed that Japanese urologists considered that inclusion criteria for active surveillance were inadequate and unexpected progression during surveillance as a major problem.38 We believe that robust evidence for a survival benefit should be established among untreated patients subdivided by age and cancer risk group to address these barriers. Robust evidence can remove patients’ and physicians’ anxiety over cancer progression, and also provide accurate information to support shared decision‐making.
The discontinuation of PSA screening among super‐elderly men, who are likely subject to overtreatment of prostate cancer, should be considered, although the clinical practice guideline published by the Japanese Urological Association has not placed an age restriction on screening with PSA.39 Meanwhile, the observed higher proportion of distant prostate cancer at diagnosis among super‐elderly patients in Japan should be focused on. This high proportion is consistent with a previous study by Suzuki et al.,40 who found that 24% of super‐elderly patients diagnosed between 1991 and 1996 had stage D2 prostate cancer (TxNxM1 or T4N0M0). In general, widespread PSA screening results in a decreased proportion of advanced prostate cancer cases due to early detection. In fact, only 12% of super‐elderly men diagnosed from 1998 to 2007 in the USA, where population‐based PSA screening is more prevalent,2 had stage D2 prostate cancer.41 Although more than 10 years have passed since the previous report in Japan,40 the proportion of advanced cancers among super‐elderly patients has remained almost unchanged. This fact implies that the prevalence of PSA screening in younger men in Japan is insufficient. Further expansion of PSA screening among younger men may provide considerable additional room for decreasing the proportion of advanced prostate cancer cases among super‐elderly patients. If the prevalence of PSA screening among younger men increases, it might be appropriate to discontinue PSA screening in super‐elderly men.
A strength of our study is its calculation of survival outcomes using a high‐quality population‐based database. This strength allowed us to estimate specific survival outcomes and potential overtreatment of super‐elderly patients in Japan. The specific survival data may play an important role in helping shared decision‐making between super‐elderly patients and physicians.
However, we recognize several important limitations. First, staging and tumor grading systems in the cancer registry were different from those commonly used in clinical settings. We were also unable to incorporate PSA values. We were therefore unable to analyze based on risk classification systems such as the D'Amico risk classification determined by PSA, Gleason score, and clinical T stage.42 These limitations were inevitable in the population‐based cancer registry analysis in exchange for the strength of our study including large representative and unbiased samples of men from throughout Japan. Nevertheless, our study showed that survival outcomes of untreated super‐elderly men with localized cancer were excellent regardless of tumor grade, an important prognosis factor. We believe that the results of the large‐scale population‐based study more accurately reflect the actual clinical practice pattern in Japan. Second, information on the comorbidity of each patient was missing. However, this paper focused on clarifying overtreatment of prostate cancer by showing excellent survival among untreated patients, and the aim may be achieved without comorbidity data for the following reason. Based on previous findings, super‐elderly men who selected observation may tend to have more comorbidities than the general population of the same age.43 If this were the case, our study would have underestimated relative survival among untreated patients. Given that the 5‐year relative survival rates among untreated super‐elderly men with localized cancer were above 100%, our findings might appropriately reveal overtreatment among super‐elderly patients. Even so, given recommendations for managing elderly men with prostate cancer according to their health status, and not according to age,44 an additional study with consideration to the general condition of super‐elderly men is required. Third, our findings might be biased by selection of the prefectures, just in case information accuracy of cancer registries is associated with intensity of cancer treatment in the prefectures. However, we believe this bias may be small because the excellent survival among untreated men with localized prostate cancer was unlikely to be influenced by variations of intensity of cancer treatment between prefectures. Finally, although 5‐year follow‐up appears somewhat short, we believe that this period is suitable for evaluating overtreatment among super‐elderly men, given that life expectancy among Japanese men aged 80 and 85 years in 2007 was 8.5 and 6.2 years, respectively.45 Additional follow‐up is warranted to confirm if our findings are also applicable to men aged 75–79 years with approximately 10 years of life expectancy.
In conclusion, more than half of super‐elderly men with localized prostate cancer may be overtreated in Japan. Considering the actual difficulty in identifying real “overtreatment” among super‐elderly men due to variation in patient characteristics, including comorbidities and treatment preferences, accumulation of evidence based on survival data among super‐elderly patients will help clarify the overtreatment groups and reduce overtreatment.
Disclosure Statement
The authors have no conflict of interest.
Abbreviations
- DCN
death certificate notification
- DCO
death certificate only
- M/I
mortality to incidence ratio
- PSA
prostate‐specific antigen
- SEER
Surveillance Epidemiology and End Results
Supporting information
Fig. S1. Twenty‐one Japanese cancer registries participated in the study of men aged 80 years and older with localized prostate cancer in Japan.
Fig. S2. Relative survival of super‐elderly men (age, ≥80 years) with localized prostate cancer, stratified by initial treatment and tumor grade.
Fig. S3. Relative survival of treated patients with localized prostate cancer stratified by tumor grade.
Table S1. Number of super‐elderly men (age, ≥80 years) with or without active treatment for prostate cancer, stratified by tumor stage and grade.
Table S2. Five‐year relative survival rates of patients with prostate cancer shown in Figures 1, 2, 3.
Acknowledgments
The authors thank all of the participants of the Monitoring of Cancer Incidence in Japan project and each cancer registry for their cooperation and provision of data. This study was supported by a Grant‐in‐Aid for Research for Promotion of Cancer Control Programs from the Ministry of Health, Labour and Welfare, Japan (grant no. H26‐political‐general‐013).
Cancer Sci 108 (2017) 1673–1680
Funding Information
Ministry of Health, Labour and Welfare, Japan (H26‐political‐general‐013).
References
- 1. Torre LA, Bray F, Siegel RL, Ferlay J, Lortet‐Tieulent J, Jemal A. Global cancer statistics, 2012. CA Cancer J Clin 2015; 65: 87–108. [DOI] [PubMed] [Google Scholar]
- 2. Zhu Y, Wang HK, Qu YY, Ye DW. Prostate cancer in East Asia: evolving trend over the last decade. Asian J Androl 2015; 17: 48–57. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Okonogi N, Katoh H, Kawamura H et al Clinical outcomes of helical tomotherapy for super‐elderly patients with localized and locally advanced prostate cancer: comparison with patients under 80 years of age. J Radiat Res 2015; 56: 889–96. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. He W, Goodkind D, Kowal P. An Aging World: 2015. Washington, DC: U.S. Government Publishing Office, 2016. [Cited 13 December 2016]. Available from URL: https://www.census.gov/content/dam/Census/library/publications/2016/demo/p95-16-1.pdf [Google Scholar]
- 5. Cooperberg MR, Lubeck DP, Meng MV, Mehta SS, Carroll PR. The changing face of low‐risk prostate cancer: trends in clinical presentation and primary management. J Clin Oncol 2004; 22: 2141–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Lu‐Yao GL, Albertsen PC, Moore DF et al Outcomes of localized prostate cancer following conservative management. JAMA 2009; 302: 1202–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Aizer AA, Gu X, Chen MH et al Cost implications and complications of overtreatment of low‐risk prostate cancer in the United States. J Natl Compr Canc Netw 2015; 13: 61–8. [DOI] [PubMed] [Google Scholar]
- 8. Cooperberg MR, Broering JM, Carroll PR. Time trends and local variation in primary treatment of localized prostate cancer. J Clin Oncol 2010; 28: 1117–23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Tyson MD, Graves AJ, O'Neil B et al Urologist‐level correlation in the use of observation for low‐ and high‐risk prostate cancer. JAMA Surg 2017; 152: 27–34. [DOI] [PubMed] [Google Scholar]
- 10. Bill‐Axelson A, Holmberg L, Ruutu M et al Radical prostatectomy versus watchful waiting in early prostate cancer. N Engl J Med 2011; 364: 1708–17. [DOI] [PubMed] [Google Scholar]
- 11. Wilt TJ, Brawer MK, Jones KM et al Radical prostatectomy versus observation for localized prostate cancer. N Engl J Med 2012; 367: 203–13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Hamdy FC, Donovan JL, Lane JA et al 10‐year outcomes after monitoring, surgery, or radiotherapy for localized prostate cancer. N Engl J Med 2016; 375: 1415–24. [DOI] [PubMed] [Google Scholar]
- 13. Dell'Oglio P, Boehm K, Trudeau V et al Survival after conservative management versus external beam radiation therapy in elderly patients with localized prostate cancer. Int J Radiat Oncol Biol Phys 2016; 96: 1037–45. [DOI] [PubMed] [Google Scholar]
- 14. Lu‐Yao GL, Kim S, Moore DF et al Primary radiotherapy vs conservative management for localized prostate cancer‐‐a population‐based study. Prostate Cancer Prostatic Dis 2015; 18: 317–24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Potosky AL, Haque R, Cassidy‐Bushrow AE et al Effectiveness of primary androgen‐deprivation therapy for clinically localized prostate cancer. J Clin Oncol 2014; 32: 1324–30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Lu‐Yao GL, Albertsen PC, Moore DF et al Fifteen‐year survival outcomes following primary androgen‐deprivation therapy for localized prostate cancer. JAMA Intern Med 2014; 174: 1460–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Sammon JD, Abdollah F, Reznor G et al Patterns of declining use and the adverse effect of primary androgen deprivation on all‐cause mortality in elderly men with prostate cancer. Eur Urol 2015; 68: 32–9. [DOI] [PubMed] [Google Scholar]
- 18. National Comprehensive Cancer Network . The NCCN Clinical Practice Guidelines in Oncology Prostate Cancer (Version 3.2016). 2016. Available from URL: [Cited 13 December 2016]. https://www.nccn.org/professionals/physician_gls/pdf/prostate.pdf
- 19. Mottet N, Bellmunt J, Bolla M et al EAU‐ESTRO‐SIOG Guidelines on Prostate Cancer. Part 1: screening, diagnosis, and local treatment with curative intent. Eur Urol 2017; 71: 618–29. [DOI] [PubMed] [Google Scholar]
- 20. Wong YN, Mitra N, Hudes G et al Survival associated with treatment vs observation of localized prostate cancer in elderly men. JAMA 2006; 296: 2683–93. [DOI] [PubMed] [Google Scholar]
- 21. Hoffman RM, Shi Y, Freedland SJ, Keating NL, Walter LC. Treatment patterns for older veterans with localized prostate cancer. Cancer Epidemiol 2015; 39: 769–77. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Wilt TJ, MacDonald R, Rutks I, Shamliyan TA, Taylor BC, Kane RL. Systematic review: comparative effectiveness and harms of treatments for clinically localized prostate cancer. Ann Intern Med 2008; 148: 435–48. [DOI] [PubMed] [Google Scholar]
- 23. Hori M, Matsuda T, Shibata A, Katanoda K, Sobue T, Nishimoto H. Cancer incidence and incidence rates in Japan in 2009: a study of 32 population‐based cancer registries for the Monitoring of Cancer Incidence in Japan (MCIJ) project. Jpn J Clin Oncol 2015; 45: 884–91. [DOI] [PubMed] [Google Scholar]
- 24. Taylor SH, Merriman KW, Spiess PE, Pisters L. Inadequacies of the current American Joint Committee on cancer staging system for prostate cancer. Cancer 2006; 106: 559–65. [DOI] [PubMed] [Google Scholar]
- 25. Dickman PW, Sloggett A, Hills M, Hakulinen T. Regression models for relative survival. Stat Med 2004; 23: 51–64. [DOI] [PubMed] [Google Scholar]
- 26. National Cancer Center, Center for Cancer Control and Information Services . Japanese cohort life table, version 2014, Tokyo, Japan: Available from URL: [Cited 13 December 2016]. http://www.mhlw.go.jp/za/0723/b09/b09.pdf [Google Scholar]
- 27. Eloranta S, Adolfsson J, Lambert PC et al How can we make cancer survival statistics more useful for patients and clinicians: an illustration using localized prostate cancer in Sweden. Cancer Causes Control 2013; 24: 505–15. [DOI] [PubMed] [Google Scholar]
- 28. Nur U, Shack LG, Rachet B, Carpenter JR, Coleman MP. Modelling relative survival in the presence of incomplete data: a tutorial. Int J Epidemiol 2010; 39: 118–28. [DOI] [PubMed] [Google Scholar]
- 29. Rubin DB. Multiple Imputation for Nonresponse in Surveys. New York: John Wiley & Sons, 1987. [Google Scholar]
- 30. Brookhart MA, Patrick AR, Dormuth C et al Adherence to lipid‐lowering therapy and the use of preventive health services: an investigation of the healthy user effect. Am J Epidemiol 2007; 166: 348–54. [DOI] [PubMed] [Google Scholar]
- 31. Miller DC, Gruber SB, Hollenbeck BK, Montie JE, Wei JT. Incidence of initial local therapy among men with lower‐risk prostate cancer in the United States. J Natl Cancer Inst 2006; 98: 1134–41. [DOI] [PubMed] [Google Scholar]
- 32. Daskivich TJ, Chamie K, Kwan L et al Overtreatment of men with low‐risk prostate cancer and significant comorbidity. Cancer 2011; 117: 2058–66. [DOI] [PubMed] [Google Scholar]
- 33. Sohn M, Jung M. Effects of public and private health insurance on medical service utilization in the National Health Insurance System: National panel study in the Republic of Korea. BMC Health Serv Res 2016; 16: 503. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Xu J, Neale AV, Dailey RK, Eggly S, Schwartz KL. Patient perspective on watchful waiting/active surveillance for localized prostate cancer. J Am Board Fam Med 2012; 25: 763–70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Taylor KL, Hoffman RM, Davis KM et al Treatment preferences for active surveillance versus active treatment among men with low‐risk prostate cancer. Cancer Epidemiol Biomarkers Prev 2016; 25: 1240–50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Davison BJ, Breckon E. Factors influencing treatment decision making and information preferences of prostate cancer patients on active surveillance. Patient Educ Couns 2012; 87: 369–74. [DOI] [PubMed] [Google Scholar]
- 37. Gorin MA, Soloway CT, Eldefrawy A, Soloway MS. Factors that influence patient enrollment in active surveillance for low‐risk prostate cancer. Urology 2011; 77: 588–91. [DOI] [PubMed] [Google Scholar]
- 38. Mitsuzuka K, Koga H, Sugimoto M et al Current use of active surveillance for localized prostate cancer: a nationwide survey in Japan. Int J Urol 2015; 22: 754–9. [DOI] [PubMed] [Google Scholar]
- 39. The Japanese Urological Association: Guideline of prostate cancer 2012: Kanehara Publishers Inc. 2012: 12–13. (in Japanese). [Google Scholar]
- 40. Suzuki H, Akakura K, Ueda T et al Clinical characteristics of prostate cancer in elderly Japanese patients 80 years of age or older. Eur Urol 2002; 41: 172–7. [DOI] [PubMed] [Google Scholar]
- 41. Scosyrev E, Messing EM, Mohile S, Golijanin D, Wu G. Prostate cancer in the elderly: frequency of advanced disease at presentation and disease‐specific mortality. Cancer 2012; 118: 3062–70. [DOI] [PubMed] [Google Scholar]
- 42. D'Amico AV, Whittington R, Malkowicz SB et al Biochemical outcome after radical prostatectomy, external beam radiation therapy, or interstitial radiation therapy for clinically localized prostate cancer. JAMA 1998; 280: 969–74. [DOI] [PubMed] [Google Scholar]
- 43. Boehm K, Dell'Oglio P, Tian Z et al Comorbidity and age cannot explain variation in life expectancy associated with treatment of non‐metastatic prostate cancer. World J Urol 2017; 35: 1031–6. [DOI] [PubMed] [Google Scholar]
- 44. Droz J‐P, Aapro M, Balducci L et al Management of prostate cancer in older patients: updated recommendations of a working group of the International Society of Geriatric Oncology. Lancet Oncol 2014; 15: e404–14. [DOI] [PubMed] [Google Scholar]
- 45. Ministry of Health, Labour and Welfare . Abridged Life Tables for Japan 2007, Tokyo, Japan: Available from URL: [Cited 13 December]. http://www.mhlw.go.jp/english/database/db-hw/lifetb07/index.html [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Fig. S1. Twenty‐one Japanese cancer registries participated in the study of men aged 80 years and older with localized prostate cancer in Japan.
Fig. S2. Relative survival of super‐elderly men (age, ≥80 years) with localized prostate cancer, stratified by initial treatment and tumor grade.
Fig. S3. Relative survival of treated patients with localized prostate cancer stratified by tumor grade.
Table S1. Number of super‐elderly men (age, ≥80 years) with or without active treatment for prostate cancer, stratified by tumor stage and grade.
Table S2. Five‐year relative survival rates of patients with prostate cancer shown in Figures 1, 2, 3.