
Fig. 4.
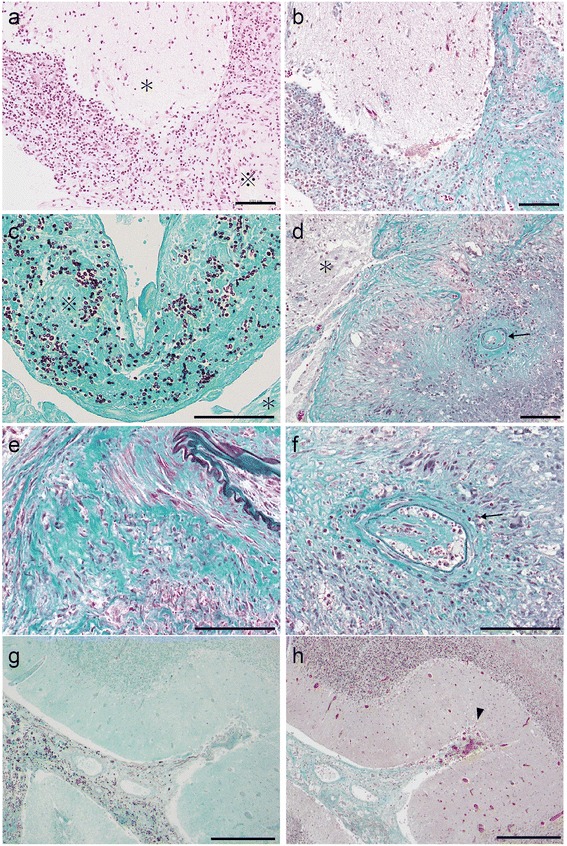
Pathological findings of the cerebellum specimen. a Hematoxylin and Eosin staining of the left cerebellar hemisphere from the surgical specimen. The subarachnoid space was heavily thickened with inflammatory cells, which is expressed as ※. The parenchyma is expressed as *. Scale bar: 100 μm. b Elastica–Masson staining at the same location as in (a). Fibrosis was widely observed in the subarachnoid space, which appears green. Scale bar: 100 μm. c Grocott staining of left cerebellar hemisphere from the surgical specimen. Fungi were observed in the subarachnoid space (※) and few fungi were observed inside the parenchyma (*). Scale bar: 100 μm. d, e, f Elastica–Masson staining of the left cerebellar hemisphere from the surgical specimen. Strong and diffuse fibrosis was observed in the subarachnoid space (e). Proliferation of endothelial cells was observed inside the inner cavity of small arteries (arrows in d, f), which implies the slow progression of arterial occlusion. Veins were rarely observed in the subarachnoid space, which indicates that they were compressed and occluded. The parenchyma is expressed as *. Scale bar: 100 μm. g Grocott staining of the deep sulcus in the left cerebellar hemisphere from the autopsy specimen. The subarachnoid space was filled with fungi not only at the surface of the cerebellar hemisphere but also in the deep sulcus. Scale bar: 500 μm. h Elastica–Masson staining at the same location as in (e). Fibrosis and thickening of the subarachnoid space was observed even in the deep sulcus of the cerebellar hemisphere. Venules from the parenchyma were frequently observed to be congested at the entry to the fibrinous subarachnoid space (arrow head). Scale bar: 500 μm