
Figure 4. Survival in a virtual clinical trial utilizing two non-cross resistant therapies.
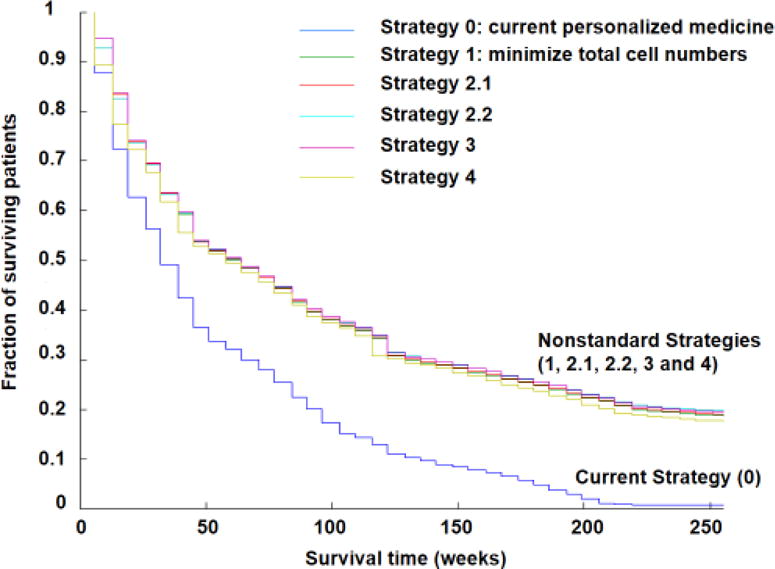
Approximately 3 million virtual patients were treated with each of these strategies. The x axis shows time (weeks) and the y axis shows surviving patient fraction. Strategy 0 (dark blue) is the current personalized medicine strategy: treatment with the best drug for the observed predominant cell type and switching to the alternative drug on tumor progression or relapse. Strategy 1 (green) minimizes total cell numbers at the next timepoint. Strategy 2.1 (red) minimizes the chance of developing doubly resistant cells at the next timepoint unless the patient has detectable disease (109 cells); in that case, total cell number is minimized. Strategy 2.2 (light blue) minimizes the chance of developing doubly resistant cells at the next timepoint unless the patient has a large disease burden (1011 cells); in that case, total cell number is minimized. Strategy 3 minimizes the total cell population unless the predicted number of doubly resistant cells at the next timepoint is ≥ 1; then the likelihood of formation of doubly resistant cells is minimized. Strategy 4 (olive) predicts the time to mortality (1013 cells) and the time to doubly resistant cells, and prioritizes the most imminent threat. Adapted from [67].