

Synopsis
The clinical use of amide proton transfer (APT) imaging is hindered by long scan times. Accuracy generally limits the use of conventional sensitivity encoding (SENSE) methods in APT, to an acceleration factor of 2. A novel variably-accelerated sensitivity encoding (vSENSE) method can provide more accurate results and therefore substantially higher overall acceleration factors than conventional SENSE. Here, vSENSE is further developed to eliminate the requirement that one fully-sampled APT frame be acquired, and extended to three dimensions (3D). Furthermore, we combine vSENSE with parallel transmit saturation, and apply it proactively to three normal volunteers and eleven patients with brain tumors.
Purpose
A novel variably-accelerated sensitivity encoding (vSENSE) method1 was proposed recently to accelerate chemical exchange saturation transfer (CEST) MRI. The vSENSE method utilized self-consistent incoherence absorption or artifact suppression (AS) strategies to improve the sensitivity maps used for SENSE2 unfolding. Here, the vSENSE method is further developed in four major aspects for APT imaging. First, the vSENSE method required one CEST/APT frame to be fully-sampled1. It is shown here that the AS algorithm can be applied to improve sensitivity using an already-accelerated frame. Second, the vSENSE method is expanded from two dimensions (2D) to 3D. Third, 3D vSENSE is applied proactively in humans to produce accurate results in healthy and brain tumor patients at accelerations of R≤4. Fourth, the vSENSE method is combined with the interleaved parallel transmit scheme3 to enable a long continuous saturation with an effective duty cycle of 100%.
Methods
Three normal volunteers and eleven brain tumor patients were scanned on a 3T Philips Achieva MRI system with a 32-channel head coil. For each participant, a SENSE reference scan was acquired using a gradient echo sequence. A 2D APT sequence was applied in 9 patients using four 2µT, 200ms block saturation pulses and a 10ms inter-block gap (52 frames with unsaturation—S0 and saturation frequencies from 14 to -8ppm stepped at 0.5ppm, where the ±3.5ppm frames were acquired with 4 averages; SENSE acceleration factor R=1; duration=2.7min). In two tumor patients and three normal volunteers, a 3D APT sequence was implemented with sixteen alternated 50ms sinc-center pulses using the interleaved parallel transmit saturation scheme3 (9 frames with S0, ±3, ±3.5, ±3.5, and ±4ppm; SENSE R=2; duration=3min). A proactive 3D vSENSE APT sequence was also applied to the normal volunteers using the same parameters except for setting R=4 for the ±3 and ±4ppm frames and R=2 for the ±3.5ppm frames. This reduced the scan-time to 2min. For each participant, conventional FLAIR4, T1w5 and “WASSR”6 (for B0 correction) sequences were also acquired as a part of the clinical protocol, which included scans with gadolinium (Gd) contrast enhancement in some cases.
Sensitivity maps were calculated from the SENSE reference scan after registration and interpolation to match the geometry to the APT scan. SENSE images were reconstructed2 with R=1, 2 or 4 constant for all frames. vSENSE images were reconstructed using the AS algorithm1 to improve the sensitivity maps using the selected image frame. For the nine 2D APT data sets from brain tumor patients, one 3.5ppm frame was selected with R=1 or 2 to generate the vSENSE sensitivity maps, both with R=2 used for the remaining seven ±3.5ppm frames and R=4 used for the other frames. This resulted in a mean retroactive R of 3.67 and 3.69, respectively. For both retroactive vSENSE on the 3D brain tumor data sets and proactive vSENSE on the 3D normal volunteer data sets, R=2 for the ±3.5ppm frames and R=4 for the other frames, leading to an average R of 3.1.
Results
Figure 1 shows conventional SENSE with R=4 (Fig. 1c, g) had a much greater error than vSENSE with R=4 (Figs. 1d, h, e, i) for the source image at 14ppm. vSENSE with R=4 yielded an error less than or comparable to that of SENSE with R=2 if the 3.5ppm frame was selected with R=1 or 2, respectively (Figs. 1h, i).
Figure 1.
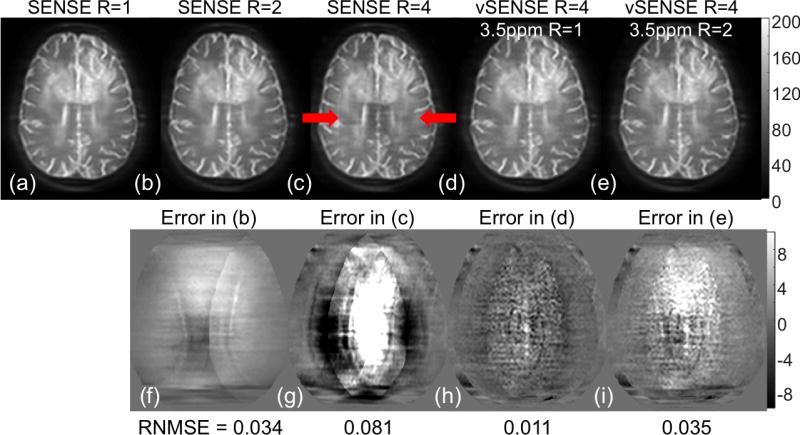
Comparison of source images at 14ppm from a brain tumor patient reconstructed with conventional SENSE (R=1 in a, R=2 in b, and R=4 in c) and vSENSE using one 3.5ppm frame (fully-sample in d, and undersampled by a factor of 2 in e) to improve sensitivity maps. The difference of accelerated SENSE and vSENSE images (b–e) from the full k-space image (a) were shown in (f–i), respectively. Red arrows indicated artifacts in the conventional SENSE R=4 image. RNMSE stands for root normalized mean squared error.
Error analysis of the nine 2D data sets showed that vSENSE with R=4 using a fully-sampled 3.5ppm frame generated a significantly smaller error than conventional SENSE (p=0.0002). In addition, the error in using vSENSE with R=4 and a 2-fold undersampled 3.5ppm frame did not differ significantly (p≈1.0) from that of conventional SENSE deployed with R=2, taking twice as long.
Figure 2 illustrates that vSENSE with either the 3.5ppm frame fully-sampled (Fig. 2d) or under-sampled (Fig. 2e) generated APTw maps that agreed with conventional SENSE with R=1 and 2 (Fig. 2a, b). Use of conventional SENSE with R=4 produced unacceptable artifacts (Fig. 2c).
Figure 2.
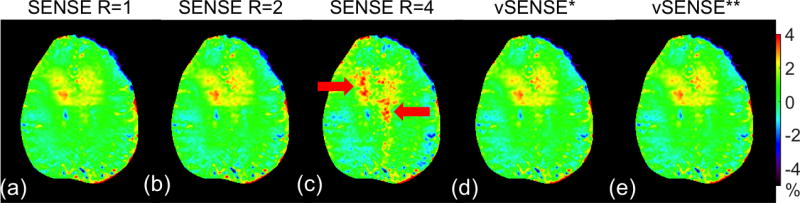
APTw image from the brain tumor patient shown in Figure 1 using conventional SENSE (R=1 in a, R=2 in b, and R=4 in c) and vSENSE (the 3.5ppm frame for improving sensitivity maps was fully-sample in d, and was undersampled by a factor of 2 in e). Red arrows indicated artifacts in the conventional SENSE R=4 results. *The mean R factor for all frames was 3.67. **The mean R factor for all frames was 3.69.
Figure 3 demonstrates that 3D proactive vSENSE with a mean R of 3.1 produced comparable APTw images to those of conventional SENSE with R=2 in a normal volunteer. Similar results were obtained for 3D retroactive vSENSE vs. conventional SENSE on a brain tumor patient in Figure 4.
Figure 3.
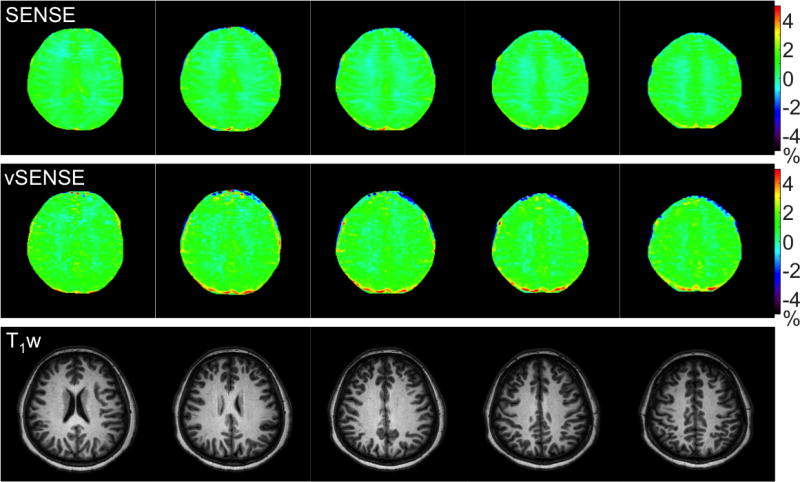
Five out of a total of fifteen APTw images from a normal volunteer using SENSE and vSENSE in conjunction with corresponding anatomical T1w images. SENSE used an R factor of 2 for all frames. vSENSE used proactive R factors of 4 for the S0, ±3ppm and ±4ppm frames, and of 2 for the ±3.5ppm frames. The mean R factor for all frames was 3.1 for vSENSE.
Figure 4.
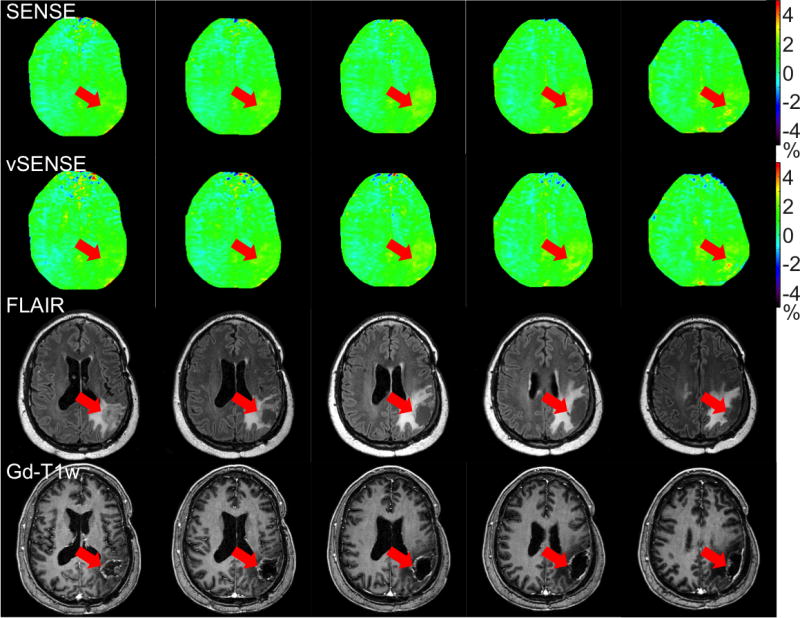
Five out of a total of fifteen APTw images from a post-treatment brain tumor patient using SENSE and vSENSE in conjunction with corresponding anatomical FLAIR and post-gadolinium T1w (Gd-T1w) images. SENSE used an R factor of 2 for all frames. vSENSE used proactive R factors of 4 for the S0, ±3ppm and ±4ppm frames, and of 2 for the ±3.5ppm frames. The mean R factor for all frames was 3.1 for vSENSE. No substantial enhancement was seen on APTw images, agreeing with the clinical diagnosis of treatment effects instead of active tumors.
Conclusions
The vSENSE method doubled the achievable acceleration factor of conventional SENSE while preserving the accuracy of APTw images. Combined with the interleaved parallel transmit saturation scheme, vSENSE should facilitate routine CEST/APT imaging of brain tumors as well as other neurological diseases.
Acknowledgments
Funding Support: NIH R01 EB007829, CA166171, EB009731, K99EB022625.
References
- 1.Zhang Y, Heo HY, Lee DH, Jiang S, Zhao X, Bottomley PA, Zhou J. Chemical exchange saturation transfer (CEST) imaging with fast variably-accelerated sensitivity encoding (vSENSE) Magn Reson Med. 2016 doi: 10.1002/mrm.26307. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Pruessmann KP, Weiger M, Scheidegger MB, Boesiger P. SENSE: sensitivity encoding for fast MRI. Magn Reson Med. 1999;42(5):952–62. [PubMed] [Google Scholar]
- 3.Keupp J, Baltes C, Harvey P, Van den Brink J, editors. Proceedings of the International Society for Magnetic Resonance in Medicine. 2011. Parallel RF transmission based MRI technique for highly sensitive detection of amide proton transfer in the human brain. [Google Scholar]
- 4.Hajnal JV, Bryant DJ, Kasuboski L, Pattany PM, De Coene B, Lewis PD, Pennock JM, Oatridge A, Young IR, Bydder GM. Use of fluid attenuated inversion recovery (FLAIR) pulse sequences in MRI of the brain. J Comput Assist Tomogr. 1992;16(6):841–4. doi: 10.1097/00004728-199211000-00001. [DOI] [PubMed] [Google Scholar]
- 5.Mugler JP, Brookeman JR. Three-dimensional magnetization-prepared rapid gradient-echo imaging (3D MP RAGE) Magn Reson Med. 1990;15(1):152–7. doi: 10.1002/mrm.1910150117. [DOI] [PubMed] [Google Scholar]
- 6.Kim M, Gillen J, Landman BA, Zhou J, van Zijl P. Water saturation shift referencing (WASSR) for chemical exchange saturation transfer (CEST) experiments. Magn Reson Med. 2009;61(6):1441–50. doi: 10.1002/mrm.21873. [DOI] [PMC free article] [PubMed] [Google Scholar]