
Fig. 7. Multimodality imaging for preoperative and intraoperative guidance and postoperative confirmation.
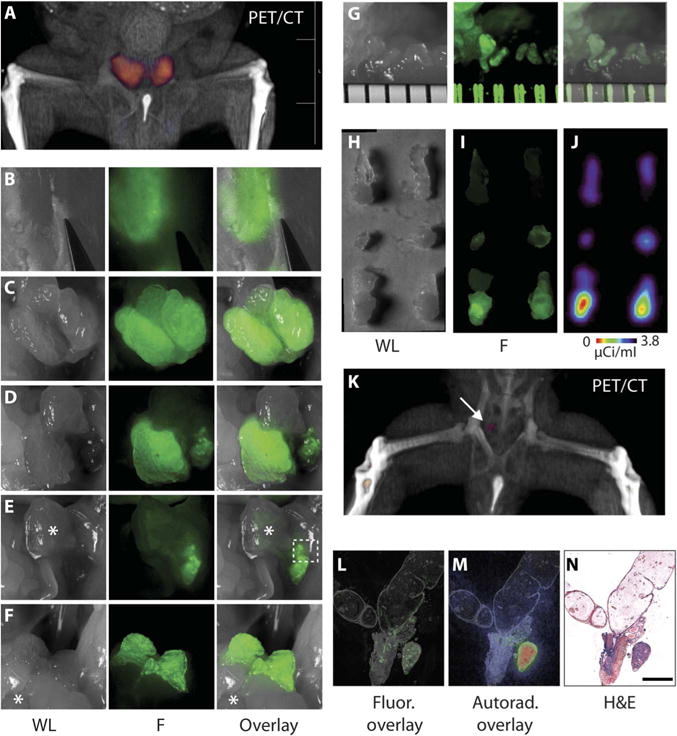
(A) Volume-rendered PET/CT demonstrates localization of signal in the prostate for preoperative planning. (B to G) White light (WL) (left), fluorescence (F) (middle), and composite (right) images obtained at different stages during dissection of the prostate. (B) Detection of fluorescence corresponding to prostate lobes through an intact peritoneum and abdomen. (C) Fluorescence signal outlines the hK2-positive tissue of the intact ventral prostate lobes. (D) An intact right ventral prostate lobe after left lobe removal. (E) Imaging after gross removal of both ventral lobes. Bladder indicated with an asterisk. (F) Delineation of intact dorsal-lateral lobes after rostral-caudal manipulation of the bladder (*). (G) Stereoscope magnification (ruler separations are about 800 μm) of area outlined in (E). (H to J) The resected prostate lobes imaged with conventional white light (H), fluorescence (I), and radio signal (J). (K) Postsurgical PET/CT reveals a small remnant focus of signal (arrow). (L and M) After excision at autopsy, seminal vesicles, urethra, and remnant tissue were sectioned and imaged by fluorescence microscopy (L) and autoradiography (M). (N) H&E stain confirmed adenocarcinoma (scale bar, 500 μm).