
Figure 1. Etiological and Pathophysiological Model of Heart Failure with Preserved Ejection Fraction.
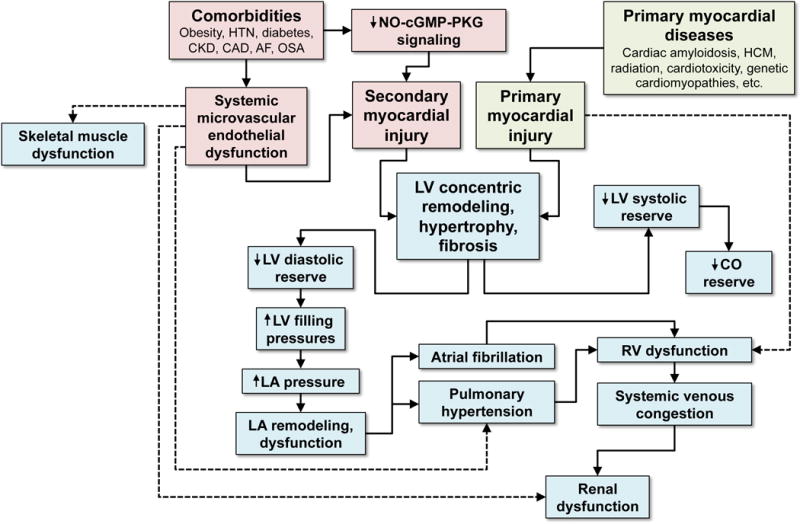
HFpEF can result from primary or secondary myocardial injury, with the latter being more typical of the syndrome. Comorbidities are thought to lead to systemic inflammation, which is associated with systemic endothelial dysfunction and decreased NO-cGMP-PKG signaling which result in secondary myocardial injury. Other diseases such as cardiac amyloidosis and HCM result in primary myocardial injury. Regardless of the cause, LV concentric remodeling and hypertrophy ensues, which results in a cascade of LV dysfunction, LA dysfunction, and RV dysfunction, ultimately leading to pulmonary and systemic venous congestion. Systemic endothelial dysfunction also likely contributes to skeletal muscle dysfunction and renal dysfunction, both of which are present in the vast majority of HFpEF patients. HTN = hypertension; CKD = chronic kidney disease; CAD = coronary artery disease; AF = atrial fibrillation; OSA = obstructive sleep apnea; NO = nitric oxide; cGMP = cyclic guanosine monophosphate; PKG = protein kinase G; HCM = hypertrophic cardiomyopathy; LV = left ventricular; LA = left atrial; RV = right ventricular; CO = cardiac output.