

Abstract
As a form of therapy, cognitive behavioral therapy (CBT) is more than a mere “toolbox.” CBT allows us to better understand how the human mind is functioning because it is based on neuroscience and experimental and scientific psychology. At the beginning, the Diagnostic and Statistical Manual of Mental Disorders (DSM) was “nontheoretical,” but nowadays (the most recent version being DSM-5), it is increasingly based on CBT paradigms (with the insertion of important notions such as cognitions and behaviors). This Brief Report presents what we currently know about generalized anxiety disorder (GAD) and how we can treat this condition by nonpharmaceutical means. In the last few years, GAD theories have evolved, becoming more precise about the cognitive functioning of GAD sufferers. Here, we look at current theoretical models and the main techniques of therapeutic care, as well as the advances in research about the “transdiagnostic” process and GAD in childhood. CBT is an effective treatment for GAD, typically leading to reductions in worry, and a study has shown that such therapy is equal to pharmaceutical treatment and more effective 6 months after study completion.
Keywords: child, cognitive behavioral therapy, generalized anxiety disorder, practice, transdiagnostic process
Abstract
La terapia cognitiva-conductual (TCC), como una forma de terapia, es más que una mera “caja de herramientas”. La TCC permite una mejor comprension de como funciona la mente humana ya que se basa en las neurociencias y en la psicología experimental y científica. El Manual Diagnóstico y Estadístico de los Trastornos Mentales (DSM) inicialmente fue “ateórico”, pero actualmente (la versión más reciente, el DSM 5) se basa cada vez más en paradigmas de TCC (con la inserción de importantes nociones tales como cognitiones y conductas). Este reporte breve presenta el conocimiento actual sobre el trastorno de ansiedad generalizada (TAG) y cómo puede ser tratada esta condición a través de medios no farmacológicos. En los últimos años, las teorías del TAG han evolucionado, Ilegando a ser más precisas acerca del funcionamiento cognitivo de quienes lo padecen. En este artículo se revisan los modelos teóricos actuales y las principales técnicas de manejo terapéutico, como también los avances en la investigación sobre el proceso “transdiagnóstico” y el TAG en la niñez. La TCC es un tratamiento efectivo para el TAG y lo característico es que reduzca las preocupaciones. Un estudio ha mostrado que dicha terapia es equivalente al tratamiento farmacológico y más efectiva a los seis meses de haber completado el estudio.
Abstract
Mode de traitement, la thérapie cognitivo-comportementale (TCC) est plus qu'une simple «boîte à outils». Basée sur les neurosciences et sur la psychologie scientifique et expérimental, la TCC nous permet de mieux comprendre le fonctionnement cognitif chez l'homme. A ses débuts, le DSM (Diagnostic and Statistical Manual of Mental Disorders) était «non théorique», mais aujourd'hui (la version la plus récente étant le DSM-5), Il se base de plus en plus sur des modèles de TCC (avec l'insertion de notions importantes comme la cognition et le comportement). Nous présentons ici brièvement nos connaissances actuelles sur l'anxiété généralisée (AG) et ses moyens de traitement non médicamenteux. Ces dernières années, les théories sur l'AG ont évolué en se précisant sur le fonctionnement cognitif des personnes qui en souffrent. Nous examinons ici les modèles théoriques actuels et les principales techniques de soin thérapeutique, ainsi que les avancées de la recherche sur le processus «transdiagnostique» et l'AG dans l'enfance. La TCC est un traitement efficace de l'AG, diminuant typiquement l'inquiétude excessive et une étude a montré qu'un tel traitement est équivalent à un traitement médicamenteux et plus efficace 6 mois après la fin de l'etude.
Current theoretical foundations
Generalized anxiety disorder (GAD) has been regarded as a primary diagnosis since 1987 (Diagnostic and Statistical Manual of Mental Disorders, third revision [DSM-III-R]). Previously, GAD had been considered an “anxiety neurosis.” Its specification as a singular disorder has allowed the recognition of factors common to anxiety disorders, for example, anxious anticipation, cognitive biases, and excessive concern. Additionally, GAD has specific factors that are not shared with other anxiety disorders, such as intolerance of uncertainty, and excessive concerns in several important areas. It is therefore a diagnosis whose conceptualization has much evolved over the last 2 decades, and recent studies on the subject suggest that the individualization of GAD will continue into the future.1
Nowadays, DSM-5 2 defines GAD as “the presence of excessive anxiety and worry about a variety of topics, events, or activities. Worry occurs more often than not for at least 6 months and is clearly excessive.” People suffering from GAD have great difficulty in controlling these worries. They may also present with edginess or restlessness, difficulty sleeping, difficulty concentrating, and an increase in muscle aches or soreness. GAD sufferers are generally burdened by the significant consequences the disorder has on their relationships or on their functioning.
In CBT, evaluation is crucial. Professionals rely on their clinical judgment, but they will also use standardized assessment tools to evaluate symptoms. 3-7 Excessive worry is the main symptom in GAD. Anxiety is almost always present in the minds of patients. The themes of concern are relatively similar to those of the normal population but are experienced in more catastrophic ways. The surrounding world is perceived with apprehension, vigilance, and pessimism (chronic feeling of insecurity, loss of contact with the experiential).
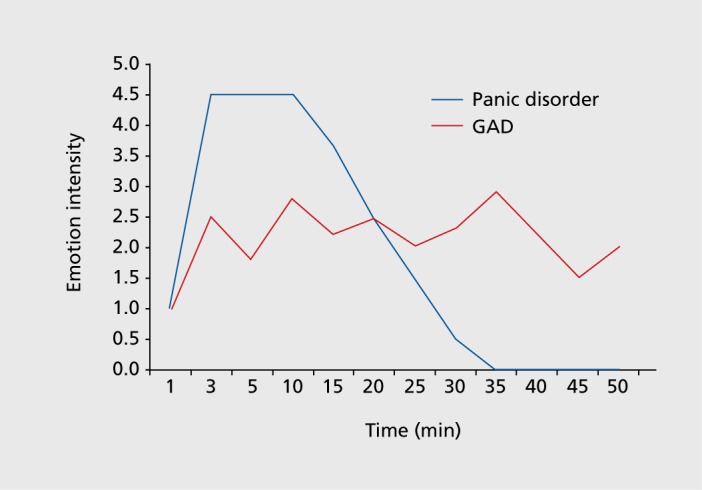
The search for reassurance is the second core element. Anxiety levels are therefore higher than in the normal population, but they are less intense and more diffuse than in a panic disorder, for example (Figure 1).
Figure 1. Difference of emotion intensity evolution over time in panic disorder versus generalized anxiety disorder. GAD, generalized anxiety disorder.
GAD affects approximately 6% of the general population in France if one considers the entire lifespan.7 The disorder is common and disabling. A recent review of epidemiological studies in Europe suggests a 12-month prevalence of between 1.7% and 3.75% (being more common in old age), and the associated functional impairment is similar to that observed with major depression.8 Comorbidities may be frequent. Indeed, 66.3% of patients present with at least one concomitant psychopathology9; in 60% of cases, major depression or another anxious disorder is present10; and 90% of GAD sufferers are suspected to have a secondary anxious disorder, such as social anxiety or panic disorder.11
Concerns described in GAD are considered as a succession of thoughts in verbal or pictorial form12-14 and not as a feeling. The emotion of anxiety will be the consequence of these worries and concerns. For instance, one might think “if I get sick, I will not be able to work anymore, I can lose my job and cannot support my family, we will find ourselves on the street...” and so on.
In order to understand the pathology, cognitive psychology attempts to represent the functioning of each disorder through models. Here, we describe two of these: Barlow's model and the model of intolerance of uncertainty.
Barlow's model15 describes a biological and psychological vulnerability to the negative elements of life. Focusing attention on potential threats fosters this vulnerability and promotes a perceived inability to control life events. Concerns have also been addressed as a way to avoid a stronger emotion. This is important from a therapeutic point of view. It explains how the disorder can maintain itself over time (maintaining factors) and which therapeutic techniques could be applied.
The model of intolerance of uncertainty16-18 is also very important. The point here is to understand that it is thought that anxiety is related to the difficulty to tolerate doubt about future events and possible negative consequences. However, why then don't people who realize that nothing bad happens end up worrying less? This could be explained by the creation of “false beliefs” or “positive beliefs” about worries. Indeed, worry is a cognitive attempt to generate ways to prevent bad events from happening and/or to prepare oneself for their occurrence. In addition, the goal of not feeling the “full” emotion is reached. Patients do not question their beliefs because they are happy that everything goes well. This is explained in the avoidance model of worry.19-20 That model also explains that in each situation, people seek to eliminate an unpleasant thought, emotion, or memory. Most often, this leads to the anxious thought ending up at the center of their attention. In addition, anxiety promotes the avoidance of mental images that are associated with greater negative emotion. Thinking about what could happen makes it possible to not suffer from emotional images that are more emotionally intense.21 Safety behaviors are then set up (frequent calls to check if everything goes well, hypervigilance about public announcement information, etc). So, whereas safety behaviors and cognitive avoidance will temporarily decrease anxiety, they will reinforce worries over time.
In summary, in the cognitive approach, worry can be used as a coping strategy because people believe in its usefulness. Indeed, some GAD sufferers affirm that it would not be normal if they didn't worry about their family or their jobs, or even that it would increase the risk that an accident would occur. Sometimes, magical thoughts are present and very resistant to change.
It is fundamental to explore and evaluate the beliefs about the function of concerns. They are powerful predisposing and maintaining factors. It is the same with patients' perception of their own emotions, which are often considered intolerable. They feel the need to suppress them as fast as they can (short-term strategy).22-26
Practical interventions
CBT as treatment for GAD includes the development of a functional analysis, providing information through psychoeducation, experimentation with new behaviors and emotions (exposition, relaxation), and a cognitive approach.
Functional analysis
Functional analysis makes it possible to specify where, when, with what frequency, with what intensity, and under what circumstances the anxious response is triggered. It is performed with the patient and integrates the factors maintaining the difficulties. This functional analysis is crucial to the smooth running of therapy because it gradually introduces important notions of psychology. It makes it possible to visualize the mental functioning of the person, which is already therapeutic in and of itself.
Psychoeducation
Psychoeducation can easily be the next step. It is generally crucial because it makes it possible to understand what the future therapeutic tools will be and facilitates the increase in motivation to change. Patients begin to think in a different way about which behaviors could be the most useful.
The emotional and behavioral approach
The emotional and behavioral approach is generally favored. The therapist tries to teach relaxation in order to instruct how to create positive emotions, not to manage negative ones. There is a double effect as follows: (i) the provision of a “psychological tool” to prepare for exposition exercises; relaxation allows desensitization of anxiogenic situations; and (ii) a balancing of the general mood by adding “cognitive break times” in thoughts and worries.
The behavioral dimension of CBT is the most important. Patients will be able to expose themselves to their own emotions and so will be able to learn how to fight maintaining factors and avoidance behaviors that perpetuate the disorder. The cognitive process that is sought is habituation. It is the acceptance of thoughts as normal and nonblocking that initiates cognitive work. An example of mental exposition is the instruction “think the worst.” This strategy allows a rapid and effective reduction in avoidance. Exposure to anxiety allows patients to remain in the presence of images related to their possible concerns (disturbing images that are usually avoided), in order to encourage emotional habituation. Patients can learn to tolerate their fears, which will allow them to think less often and less intensely about their worries.
The cognitive approach
The cognitive approach often begins with a self-observation that patients will carry out on their own thoughts. Can the thoughts be spotted? Can patients isolate them from emotions? The aim of the cognitive work is to help patients take a step back from their automatic thoughts and to be disjointed from those worries. The third wave in CBT (mindfulness) adopted this principle to create its therapeutic program with a different form.
In a second step, therapy tends to modify the content of thoughts to reach a more objective evaluation of situations. The goal is to struggle against cognitive biases, such as overgeneralization or maximization of danger. A second evaluation of situations is possible by looking for objective indicators that allow relativizing. It is also possible to evaluate the consequences of worry and to understand subtle avoidance. The therapist tries to help patients to fully treat anxious anticipations, make them aware of danger patterns, and propose alternatives to catastrophism (overestimation of risk).27
GAD in children and the transdiagnostic process
Children, too, can be worried in a pathological way. Anxieties are normal during development, but with poor emotional management they can become problematic. Always considering the “what if?” they ask a lot of questions to be sure and certain and sometimes they try to predict every possible scenario. Attentional focus on the threat appears to be a bias predisposing to GAD.28,29 Prompt treatment would seem important to prevent this “cognitive habit” from becoming anchored because intolerance of uncertainty can be the “fuel” of anxiety.30
Children with GAD show difficulty concentrating, and they are always thinking about what's next. They need reassurance and approval for small steps and avoid a lot of uncertain situations. They try to minimize risks. They can present with perfectionism, a great fear of making mistakes and a fear of criticism. They also show metacognitive bias by thinking that worries will prevent tragedies.
A child with GAD can look like he or she has depression, whereas the real problem is closer to inhibition and resignation. Psychological work with children and adolescents requires a lot of imagination. Clinicians always need to create educational support and adapt psychiatric classification to children.
Conclusion
CBT as a treatment for GAD has been established as an excellent way to change pathological worries into normal worries. A lot of research must still be done to improve therapeutic tools that facilitate distancing oneself from anxious thoughts. Current science has achieved a good understanding of psychological mechanisms in GAD, and further research in transdiagnostic fields may provide new approaches to GAD treatment.
Acknowledgments
The author declares no conflict of interest.
REFERENCES
- 1.Haute Autorite de Sante. Affections psychiatriques de longue duree. Troubles anxieux graves. Paris, France: HAS; . 2007 [Google Scholar]
- 2.American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Arlington, VA: American Psychiatric Association; . 2013 [Google Scholar]
- 3.Brown TA., Barlow DH. Treatments That Work: Anxiety and Related Disorders interview Schedule for DSM-5. New York, NY: Oxford University Press; 2014 [Google Scholar]
- 4.First MB., Spitzer RL., Gibbon M., Williams JB. Structured Clinical Interview for DSM-IV(SCID). New York, NY: Biometrics Research, New York State Psychiatric Institute; 1998 [Google Scholar]
- 5.Silverman WK., Albano AM. Anxiety Disorders Interview Schedule for DSM-iV: Child Version, Child And Parent Interview Schedules. San Antonio, TX: Psychological Corporation; 1996 [Google Scholar]
- 6.Spitzer R., Kroenke K., Williams J., Lowe B. A brief measure for assessing generalized anxiety disorder. Arch Intern Med. 2006;166(10):1092–1097. doi: 10.1001/archinte.166.10.1092. [DOI] [PubMed] [Google Scholar]
- 7.Dugas MJ., Freeston MH., Lachance S., et al The worry and anxiety questionnaire: initial validation in nonclinical and clinical samples. Paper presented at: World Congress of Behavioral and Cognitive Therapies; July 1995; Copenhagen, Denmark. [Google Scholar]
- 8.Agence Nationale d'Accréditationale d'Accréditation et d'Evaluation en Santé. Diagnostic et prise en charge en ambulatoire du trouble anxieux généralisé de l'adulte. Recomm Pour La Prat Clin. 2001:1–9. [Google Scholar]
- 9.Wittchen HU., Zhao S., Kessler RC., Eaton WW. DSM-III-R generalized anxiety disorder in the National Comorbidity Survey. Arch Gen Psychiatry. 1994;51(5):355–364. doi: 10.1001/archpsyc.1994.03950050015002. [DOI] [PubMed] [Google Scholar]
- 10.Nutt D., Argyropoulos S., Hood S., Potokar J. Generalized anxiety disorder: a comorbid disease. Eur Neuropsychopharmacol.. 2006;16( suppl 2):S109–S118. doi: 10.1016/j.euroneuro.2006.04.003. [DOI] [PubMed] [Google Scholar]
- 11.Barlow DH., Rapee RM., Brown TA. Behavioral treatment of generalized anxiety disorder. Behav Ther. 1992;23(4):551–570. [Google Scholar]
- 12.Lader M. Generalized anxiety disorder. Encyclopedia Psychopharmacol.. 2015:699–702. [Google Scholar]
- 13.Borkovec TD., Robinson E., Pruzinsky T., DePree JA. Preliminary exploration of worry: some characteristics and processes. Behav Res Ther. 1983;21(1):9–16. doi: 10.1016/0005-7967(83)90121-3. [DOI] [PubMed] [Google Scholar]
- 14.Macleod AK., Williams JM., Bekerian DA. Worry is reasonable: the role of explanations in pessimism about future personal events. J Abnorm Psychol. 1991;100(4):478–486. doi: 10.1037//0021-843x.100.4.478. [DOI] [PubMed] [Google Scholar]
- 15.Barlow DH., Di Nardo PA. The diagnosis of generalized anxiety disorder: development, current status, and future directions. In Rapee RM, Barlow DH, eds. Chronic Anxiety: Generalized Anxiety Disorder, and Mixed Anxiety-Depression. New York, NY: Guilford Press; 1991:95–118. [Google Scholar]
- 16.Mogg K., Mathews A., Weinman J. Memory bias in clinical anxiety. J Abnorm Psychol. 1987;96(2):94–98. doi: 10.1037//0021-843x.96.2.94. [DOI] [PubMed] [Google Scholar]
- 17.Dugas MJ., Freeston MH., Ladouceur R. Intolerance of uncertainty and problem orientation in worry. Cogn Ther Res. 1997;21(6):593–606. [Google Scholar]
- 18.Dugas MJ., Gagnon F., Ladouceur R., Freeston MH. Generalized anxiety disorder: a preliminary test of a conceptual model. Behav Res Ther. 1998;36(2):215–226. doi: 10.1016/s0005-7967(97)00070-3. [DOI] [PubMed] [Google Scholar]
- 19.Borkovec TD. The nature, functions, and origins of worry. In Davey GC, Tallis F, eds. Worrying: Perspectives on Theory, Assessment and Treatment. Oxford, UK: Wiley; 1994:5–33. [Google Scholar]
- 20.Borkovec TD., Alcaine O., Behar ES. Avoidance theory of worry and generalized anxiety disorder. In Heimberg R, Mennin D, Turk C, eds. Generalized Anxiety Disorder: Advances in Research and Practice. New York, NY: Guilford press; 2004:77–108. [Google Scholar]
- 21.Hoyer J., Becker ES., Roth WT. Characteristics of worry in GAD patients, social phobics, and controls. Depress Anxiety. 2001;13(2):89–96. doi: 10.1002/da.1021. [DOI] [PubMed] [Google Scholar]
- 22.Mennin DS., Turk CL., Heimberg R., Carmin C. Focusing on the regulation of emotion: a new direction for conceptualizing and treating generalized anxiety disorder. In: Reinecke MA, Clark DA, eds. Cognitive Therapy Across the Lifespan: Evidence and Practice. New York, NY: Cambridge University Press; 2004:60–89. [Google Scholar]
- 23.Cisler JM., Olatunji BO., Feldner MT., Forsyth JP. Emotion regulation and the anxiety disorders: an integrative review. J Psycopathol Behav Assess. 2010;32(1):68–82. doi: 10.1007/s10862-009-9161-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Thayer JF., Lane RD. A model of neurovisceral integration in emotion regulation and dysregulation. J Affect Disord. 2000;61(3):201–216. doi: 10.1016/s0165-0327(00)00338-4. [DOI] [PubMed] [Google Scholar]
- 25.Dugas M., Ladouceur R. Treatment of GAD. Targeting intolerance of uncertainty in two types of worry. Behav Modif. 2000;24(5):635–657. doi: 10.1177/0145445500245002. [DOI] [PubMed] [Google Scholar]
- 26.Dugas MJ., Letarte H., Rheaume J., et al Worry and problem solving: evidence of a specific relationship. Cogn Ther Res. 1995;19:109–120. [Google Scholar]
- 27.Cottraux J. Les Thérapies Comportementales et Cognitives. 3rd ed. Paris, France: Masson; . 1998 [Google Scholar]
- 28.Waters AM., Bradley BP., Mogg K. Biased attention to threat in paediatric anxiety disorders (generalized anxiety disorder, social phobia, specific phobia, separation anxiety disorder) as a function of “distress” versus “fear” diagnostic categorization. Psychol Med. 2014;44(3):607–616. doi: 10.1017/S0033291713000779. [DOI] [PubMed] [Google Scholar]
- 29.Armstrong T., Zald DH., Olatunji BO. Attentional control in OCD and GAD: specificity and associations with core cognitive symptoms. Behav Res Ther. 2011;49(11):756–762. doi: 10.1016/j.brat.2011.08.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Einstein, Danielle A. Extension of the transdiagnostic model to focus on intolerance of uncertainty: a review of the literature and implications for treatment. Clin Psychol Sci Pract. 2014;21(3):1468–2850. doi: 10.1111/cpsp.12077. [DOI] [PMC free article] [PubMed] [Google Scholar]