

Abstract
Objective
To evaluate the adequacy of ultrasonography (US) and computed tomography (CT) in the assessment of thyroid cartilage invasion in patients with airway cancer.
Materials and methods
Sixty-two consecutive patients referred to our institute underwent US and CT to stage laryngeal (n = 27) or hypopharyngeal (n = 35) cancer in this prospective study. Two radiologists, who were blinded to the patients’ clinical histories and histopathology, evaluated thyroid cartilage invasion on US and CT separately and independently. Fifty-eight of the 64 patients (90%) underwent surgery. The histopathologic findings were used as the standard of reference for comparison and statistical analysis.
Results
For thyroid cartilage invasion, the detection rate on CT and US was 98%. CT achieved a sensitivity of 91% and a specificity of 75%, while US attained a sensitivity of 98% and a specificity of 75%. The difference between CT and US in terms of sensitivity was not statistically significant.
Conclusion
US and CT have high diagnostic performance in evaluating thyroid cartilage invasion. US is more sensitive than CT in diagnosing invasion of the thyroid cartilage; however, the difference is not statistically significant. US can be used to solve the diagnostic dilemma of the presence or absence of cartilage invasion when CT is inconclusive, as CT is more widely used in staging laryngeal and hypopharyngeal cancers.
Keywords: US, CT, Thyroid cartilage invasion, Ultrasonography, Computed tomography
Sommario
Obiettivo
Valutazione dell’adeguatezza dell’ecografia e della TC nella caratterizzazione dell’invasione della cartilagine tiroidea in pazienti con neoplasie delle vie aeree.
Materiali e Metodi
Questo studio prospettico è stato condotto su 62 pazienti consecutivi che sono stati sottoposti ad ecografia e TC per la stadiazione di tumori laringei (n = 27) o ipolaringei (n = 35). Due radiologi hanno valutato l’invasione della cartilagine tiroidea tramite ecografia e TC separatamente ed indipendentemente, senza essere a conoscenza dell’anamnesi dei pazienti e dei dati istologici. 58 dei 64 pazienti (90%) sono stati sottoposti a trattamento chirurgico. I risultati istologici sono stati utilizzati come riferimento per il confronto e per l’analisi statistica.
Risultati
Il tasso di rilevamento di invasione della cartilagine tiroidea è risultato del 98% per la TC e l’ecografia. La TC ha mostrato una sensibilità del 91% ed una specificità del 75%, mentre l’ecografia una sensibilità del 98% ed una specificità del 75%. La differenza tra TC ed ecografia in termini di sensibilità e specificità non è risultata statisticamente significativa.
Conclusioni
L’ecografia e la TC sono entrambe una buona performance diagnostica nella valutazione dell’invasione della cartilagine tiroidea. La differenza non è statisticamente significativa. L’ecografia può essere utilizzata per confermare la presenza o l’assenza di invasione della cartilagine tiroidea quando la TC non risulta diagnostica, dal momento in cui la TC è più frequentemente utilizzata nella stadi azione dei tumori laringei ed ipolaringei.
Introduction
A suitable treatment strategy for laryngeal and hypopharyngeal cancer is based on the stage of the disease at the initial assessment [1]. An unambiguous determination of cartilage invasion is important for determining the appropriate management of laryngeal and hypopharyngeal cancers. Preserving the larynx is intended in early stages with no cartilage invasion. In disease with focal cartilage invasion, function-preserving partial laryngectomy or chemoradiotherapy has been introduced [2–4]. An advanced stage, with apparent cartilage invasion, may require total laryngectomy [2, 5, 6].
Laryngoscopy, computed tomography (CT) and magnetic resonance imaging (MRI) are frequently used to diagnose the disease and determine its staging [7]. Laryngoscopy is limited to evaluation of the internal extent of the disease. CT and MRI provide details on the internal and external extent of the disease. MRI shows better soft tissue resolution, but is limited by availability, high cost and longer scanning times. CT is widely used and is an accepted method for suggesting thyroid cartilage invasion, but nevertheless presents challenges [8]. The different proportions of hyaline cartilage in thyroid cartilage vary its appearance on CT and produce variable CT values. Non-ossified cartilage and tumours resemble each other, having approximate CT values of 100 HU [9, 10], making them almost inseparable, especially when the tumour is located adjacent to the non-ossified cartilage.
Calcified thyroid cartilage and air within the laryngeal cavity pose a problem in using US as a modality in evaluating the larynx and hypopharynx [11]. Despite the hurdles, multiple attempts have been made to use ultrasonography in this area, with reasonable success. Few studies have used non-invasive and real-time imaging features of US to evaluate laryngeal and hypopharyngeal tumours, succeeding in proving that US could assist tumour staging in patients with advanced laryngeal cancer [12–14].
Whether ultrasonography has a comparable ability to evaluate thyroid cartilage invasion is worth studying as a complimentary and contributory imaging method to MRI or CT. The purpose of this article was to investigate the usefulness of ultrasonography in assessing thyroid cartilage invasion in laryngeal or hypopharyngeal cancer compared with CT and the pathological findings.
Methods and materials
Study population
Our institutional review board approved this prospective study. From February 2011 to February 2013, 62 consecutive patients with biopsy-proven laryngeal or hypopharyngeal carcinoma were examined using both CT and US before treatment at our hospital. Written informed consent was taken from each patient. Of these patients, four were excluded because they had radiation therapy and/or chemotherapy without surgery after endoscopic biopsy, and the remaining 58 patients having resection were enrolled in the study.
The median interval between CT/US diagnosis and surgery was 7 days (range 1–20 days). In the 58 patients included in our study who underwent surgery, the presence or absence of thyroid cartilage invasion on CT and US was recorded. These CT and US results were compared with each other and the histopathologic findings. Histopathology (HPE) served as the standard of reference.
CT protocol
For all the CT examinations, a spiral CT scanner (SOMATOM EMO 6, Siemens, Germany) was used. Contrast-enhanced computed tomography (CECT) of the neck was performed on each patient. In all the patients, a 3-mm-thick axial scan was performed from the skull base to the thoracic inlet before and after intravenous administration of 60–100 ml of non-ionic contrast agent [Iomeprol (Iomeron 300), Bracco, Italy]. Contiguous sagittal and coronal images were reconstructed with both soft tissue and bone algorithms. Each CT scan was read by an oncoradiologist with more than 7 years of experience. The radiologist was aware of the biopsy-proven diagnosis of laryngeal or hypopharyngeal cancer but was unaware of the clinical and US findings. Patients with and without thyroid cartilage invasion (Fig. 1) on CT were segregated. The patients with thyroid cartilage invasion were further classified as having major or minor invasion. Minor invasion (Fig. 2) was considered present when there was clear erosion of the cartilage or asymmetric sclerotic changes with suspicious erosion in at least two planes. Cartilages with asymmetric sclerotic changes without suspicion of erosion in two planes were classified as negative because these changes could represent reactive changes [10, 15]. For major thyroid cartilage invasion (Fig. 5a–d), the criteria were lysis of the cartilage or extralaryngeal spread of the tumour.
Fig. 1.
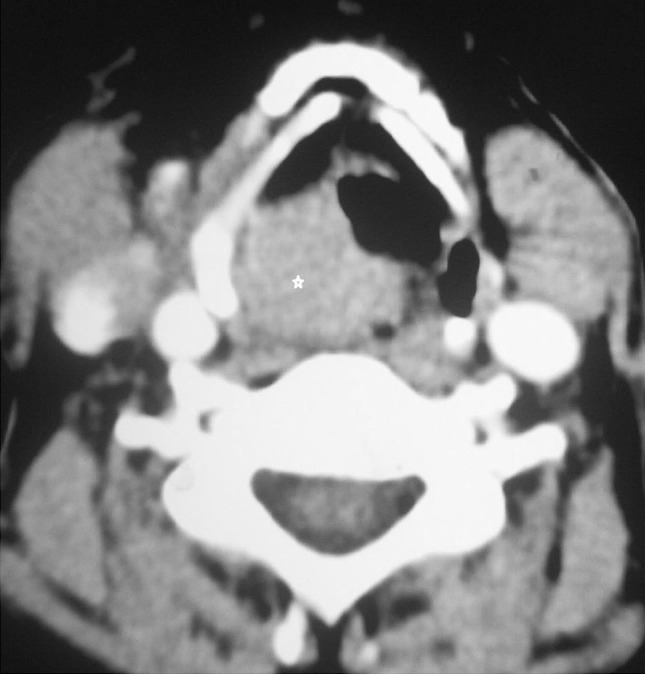
Axial CT image of right pyriform sinus cancer, marked by a star, in a 45-year-old male patient. There is no thyroid cartilage invasion on CT
Fig. 2.
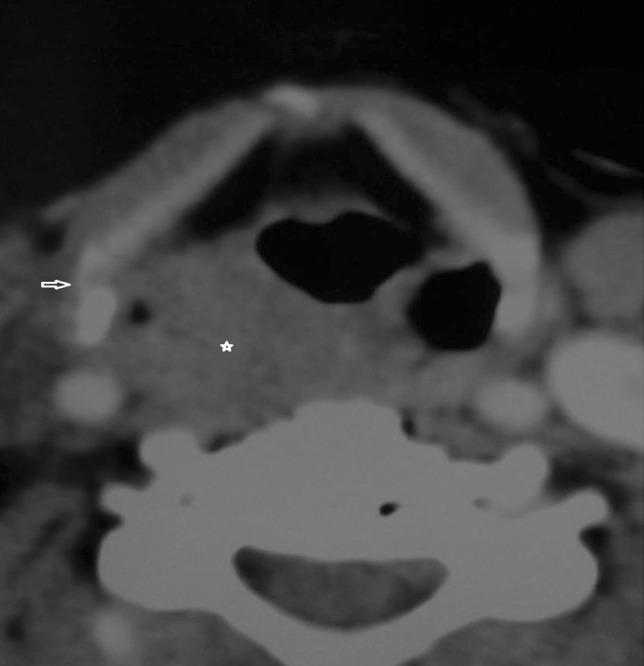
Axial CT image of a 56-year-old patient with minor thyroid cartilage erosion, shown by the arrow. The star marks the tumour
Fig. 5.

Axial CT of a large pyriform sinus growth shows extralaryngeal spread of the tumour, marked by stars. The thyroid cartilage also shows erosions. a, b Transverse US scan of a large laryngeal tumour shows thyroid cartilage erosion (arrows) and extralarngeal tumour spread (stars). c Gross specimen of the same patient, having a large pyriform sinus tumour with extralaryngeal spread. d Hematoxylin and eosin stain (×20, low power) of the same patient, showing thyroid cartilage invasion
Ultrasound protocol
A predetermined, systematic, focused ultrasound technique was followed in each patient using a high-resolution US machine (TOSHIBA NEMIO 30 SSA-550A, Toshiba Medical Systems, Japan). The sonologist performing the US had more than 7 years of experience in head and neck ultrasound and was blinded to the CT and clinical findings, but was aware that the patients were biopsy-proven cases of hypopharyngeal or laryngeal cancer. The variable appearance of thyroid cartilage on US necessitated the use of a systematic US technique where the patient was examined in the supine position with the neck extended using a high-resolution probe (7–12 MHz). The tumour was first identified, followed by the thyroid cartilage. The relationship between the tumour and the cartilage was assessed. The thyrohyoid and cricothyroid membranes allowed good acoustic windows for completely calcified thyroid cartilages. Erosion of the thyroid cartilage was indicated by the interruption of the inner and/or outer membranes, that normally are hyperechoic lines on ultrasonography images, and the replacement of the central medulla by hypoechoic tumours [16]. When the lesion was not detected on the US study, it was further excluded for evaluation of invasion. Similar to CT, each patient was segregated into negative (Fig. 3) or positive based on whether there was cartilage invasion. Minor invasion (Fig. 4) recorded subtle erosions and the relative immobility of the thyroid cartilage with respect to the hypoechoic tumour. The major invasion (Fig. 5a–d) was considered when extralaryngeal spread and clear lysis of the cartilage were identified.
Fig. 3.
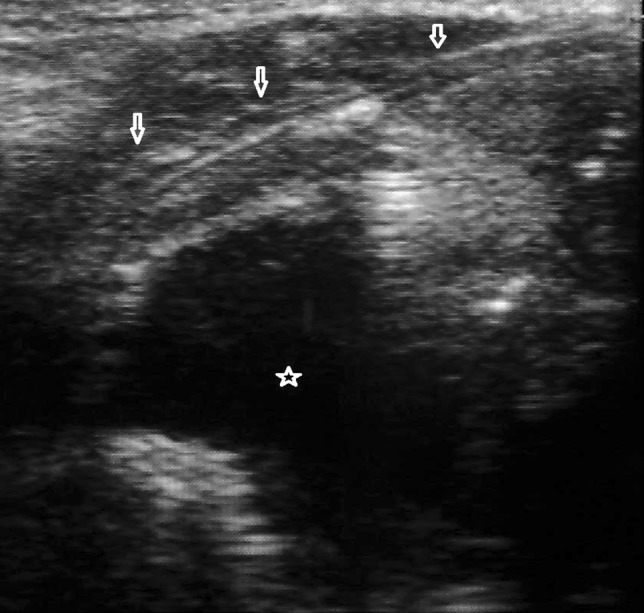
Transverse US image of right pyriform sinus cancer shows no invasion of the thyroid cartilage with maintained echogenic fat plane. The arrows point to the thyroid cartilage and the star marks the hypoechoic growth
Fig. 4.
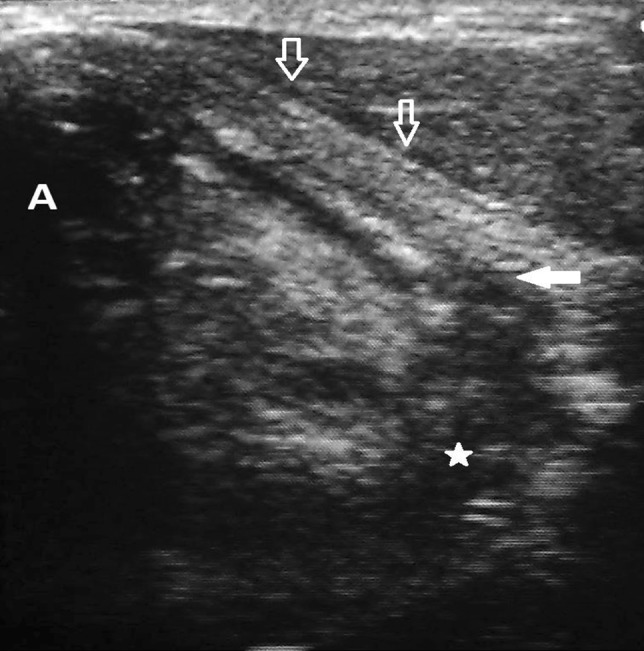
Transverse US image shows minor thyroid cartilage invasion. The arrows mark the thyroid cartilage, the solid arrow points to the focal erosion of the thyroid cartilage by the tumour, marked by a star. A is the airway
Using histopathologic findings as the reference standard, the performance of CT and US was evaluated individually in terms of detection rate, sensitivity and specificity. Fisher’s exact test was used to identify if there was any statistically significant difference between CT and US in assessing thyroid cartilage invasion.
Results
Fifty-eight of the 62 patients (93.5%) underwent surgical resection. Four of them underwent radiation therapy, chemotherapy or both. These patients were excluded from the study group. The cohort who underwent surgery included 53 males and 5 females, aged 33–81 years [mean ± standard deviation (SD), 52.1 ± 11.0 years]. Twenty-seven of the 62 patients (43.5%) had laryngeal cancer and 35 patients (56.4%) had hypopharyngeal carcinoma. Squamous cell carcinoma was histopathologically confirmed with endoscopic biopsy in all the patients.
For thyroid cartilage invasion, the detection rate on CT and US was 98%. The correlation between CT and HPE findings is shown in Table 1. The correlation between US and HPE findings is shown in Table 2.
Table 1.
Correlation between CT and HPE
| Histopathology findings | ||||
|---|---|---|---|---|
| Major invasion | Minor invasion | No invasion | Total | |
| CT findings | ||||
| Major invasion | 28 | 28 | ||
| Minor invasion | 1 | 20 | 5 | 26 |
| No invasion | 1 | 3 | 4 | |
| Total | 29 | 21 | 8 | 58 |
Table 2.
Correlation between CT and HPE findings
| Histopathology findings | ||||
|---|---|---|---|---|
| Major invasion | Minor invasion | No invasion | Total | |
| US findings | ||||
| Major invasion | 28 | 28 | ||
| Minor invasion | 1 | 20 | 4 | 25 |
| No invasion | 1 | 4 | 5 | |
| Total | 29 | 21 | 8 | 58 |
Statistical formula values at 95% CI (confidence limit) for thyroid cartilage invasion detected on CT when compared to the reference standard HPE are:
Sensitivity: 90.74% (79.70–96.92%).
Specificity: 75.00% (19.41–99.37%).
Positive likelihood ratio: 3.63 (0.66–19.86).
Negative likelihood ratio: 0.12 (0.05–0.34).
Positive predictive value: 98.00% (89.35–99.95%).
Negative predictive value: 37.50% (8.52–75.51%).
Statistical formula values at 95% CI for thyroid cartilage invasion detected on US when compared to the reference standard HPE are:
Sensitivity: 98.00% (89.35–99.95%).
Specificity: 75.00% (34.91–96.81%).
Positive likelihood ratio: 3.92 (1.18–13.03).
Negative likelihood ratio: 0.03 (0.00–0.19).
Positive predictive value: 96.08% (86.54% to 99.52%).
Negative predictive value: 85.71% (42.13–99.64%).
The above analysis was made using MedCalc statistical software.
The difference between US and CT in terms of sensitivity was not statistically significant (P > 0.05) using Fisher’s exact test.
Discussion
In the current study, we compared the diagnostic performance of CT and US with each other and HPE regarding thyroid cartilage invasion in laryngeal or hypopharyngeal cancers. This is particularly important for management decision making when function-preserving therapy is being contemplated because fewer false-positive results mean fewer avoidable laryngectomies.
During the early 1990s, CT obtained a high specificity of 87–97% and lesser sensitivity in the evaluation of thyroid cartilage invasion [17, 18]. In the late 1990s, criteria of erosion, lysis and extralaryngeal spread were introduced [10] and sensitivity of 71% and specificity of 83% were attained. After major technological advances in CT machines, Li et al. [19] reported a sensitivity of 85% and a specificity of 75% with multidetector CT. In our study, we used the published criteria for cartilage invasion and multidetector CT and achieved a sensitivity of 91%, specificity of 75%, positive predictive value of 98% and negative predictive value of 38%. However, in a recent review article by Adolphs et al. [26], four studies were included in the final analysis. Only one study examined the positive predictive value and negative predictive value for invasion of any laryngeal cartilage, and they were 87 and 56%, respectively. The positive predictive value and negative predictive value for thyroid cartilage invasion were investigated in three studies and ranged from 44 to 80%, and from 85 to 100%, respectively. The results of the negative predictive value and positive predictive value of this study and our study differ because we used a small sample group in our study.
In our study, we also provide evidence that ultrasonography could supply valuable information on the diagnosis of thyroid cartilage invasion. We found that ultrasonography findings were comparable to CT findings. Both the sensitivity and specificity were high. US provided confident, correct diagnosis of negative invasion in one of our cases where CT suggested minor invasion. US attained a positive predictive value of 96% and a negative predictive value of 86%.
Calcification of thyroid cartilage and artefacts caused by air within the laryngeal cavities provide challenges during US examinations. Furthermore, laryngeal and hypopharyngeal cancers are more common in males [20], where the thyroid cartilage calcification occurs earlier and is more complete than in females [21]. However, 50.0% or less calcification occurs in 40.0% of males, which makes a satisfactory examination of all or part of the laryngeal structures in 92.1–98.0% of them possible [22]. The uncalcified areas, the thyrohyoid and cricothyroid membranes, provided a suitable ultrasound window. In our study, these acoustic windows helped us reach a high sensitivity and specificity using US in detecting thyroid cartilage invasion, in which the male population was 91.3% (53 of 58). In addition, the laryngeal, oropharyngeal and hypopharyngeal regions could be visualized much better because of the exclusion of air by the tumour itself, which was also proven in our previous studies with tongue and hypopharyngeal carcinoma [14, 23].
The detection rate and specificity with CT and US were the same. US was more sensitive (98%) than CT; however, the difference was statistically insignificant (P > 0.05). The increased sensitivity of US was mainly due to its ability to clearly visualize the fat plane between the tumour and cartilage and the relative movement of the thyroid cartilage independent of the tumour, confidently suggesting negative invasion in one case. These results suggest that ultrasonography has a satisfying detection rate for laryngeal cancer, even in male adults with thyroid cartilage calcification, and it can be used as a complimentary modality to CT when in doubt of minor cartilage invasion.
MRI is proved to be more sensitive than CT for detecting cartilage invasion (sensitivity up to 96%) [24]. However, there are false-positive results due to peritumoural inflammation. Inflammatory changes are common in the thyroid cartilage, and the specificity of MR imaging for detecting invasion of the thyroid cartilage is only 56–65% [18, 24]. MR imaging is compromised by motion artefacts and lacks thin sections. Furthermore, MRI is generally expensive and not available widely. We did not use MRI in our study.
Our study had some limitations. First, the number of cases in this study was relatively small. Further studies with a bigger population with histologic findings are needed to substantiate a clinical effect. Second, only one examiner scanned the larynx, leading to issues with reproducibility and interobserver reliability. Considering that it is not difficult for an examiner to perform ultrasonography examination of the laryngeal area after training [25], this could be acceptable. The use of contrast-enhanced US and MRI for comparison remains areas of scope for future research.
Conclusion
Both US and CT have high diagnostic performance in evaluating thyroid cartilage invasion. US is more sensitive than CT in diagnosing invasion of the thyroid cartilage. The difference is not statistically significant. US can be used to solve the diagnostic dilemma of the presence or absence of cartilage invasion when CT is inconclusive, as CT is more widely used in staging laryngeal and hypopharyngeal cancers.
Therefore, US is a dependable modality for imaging the thyroid cartilage invasion in laryngeal and hypopharyngeal cancers. It can be used as a supplementary and complimentary method, along with CT, for conclusively detecting pre-operative thyroid cartilage invasion, helping in directing treatment strategy.
Compliance with ethical standards
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All procedures performed involving the human participants were in accordance with the ethical standards of the institutional committee and with the 1964 Helinski declaration and its amendments or comparable ethical standards. Written informed consent was taken from each patient.
Informed consent
Informed Consent was obtained from all the patients.
References
- 1.Marur S, Forastiere AA. Head and neck cancer: changing epidemiology, diagnosis, and treatment. Mayo clin proc. 2008;83(4):489–501. doi: 10.4065/83.4.489. [DOI] [PubMed] [Google Scholar]
- 2.Pfister DG, Laurie SA, et al. American Society of Clinical Oncology clinical practice guideline for the use of larynx-preservation strategies in the treatment of laryngeal cancer. J Clin Oncol. 2006;24(22):3693–3704. doi: 10.1200/JCO.2006.07.4559. [DOI] [PubMed] [Google Scholar]
- 3.Forastiere AA, Goepfert H, Maor M, et al. Concurrent chemotherapy and radiotherapy for organ preservation in advanced laryngeal cancer. N Engl J Med. 2003;349(22):2091–2098. doi: 10.1056/NEJMoa031317. [DOI] [PubMed] [Google Scholar]
- 4.Hoffman HT, Porter K, Karnell LH, et al. Laryngeal cancer in the United States: changes in demographics, patterns of care, and survival. Laryngoscope. 2006;116(9 Pt 2 Suppl 111):1–13. doi: 10.1097/01.mlg.0000236095.97947.26. [DOI] [PubMed] [Google Scholar]
- 5.Castelijns JA, Becker M, Hermans R. Impact of cartilage invasion on treatment and prognosis of laryngeal cancer. Eur Radiol. 1996;6(2):156–169. doi: 10.1007/BF00181135. [DOI] [PubMed] [Google Scholar]
- 6.Rodriguez CP, Adelstein DJ, Rybicki LA, et al. Clinical predictors of larynx preservation after multiagent concurrent chemoradiotherapy. Head Neck. 2008;30(12):1535–1542. doi: 10.1002/hed.20902. [DOI] [PubMed] [Google Scholar]
- 7.Zbären P, Becker M, Läng H. Staging of laryngeal cancer: endoscopy, computed tomography and magnetic resonance versus histopathology. Eur Arch Otorhinolaryngol. 1997;254:S117–S122. doi: 10.1007/BF02439740. [DOI] [PubMed] [Google Scholar]
- 8.Kuno H, Onaya H, Iwata R, Kobayashi T, Fujii S, Hayashi R, et al. Evaluation of cartilage invasion by laryngeal and hypopharyngeal squamous cell carcinoma with dual-energy CT. Radiology. 2012;265(2):488–496. doi: 10.1148/radiol.12111719. [DOI] [PubMed] [Google Scholar]
- 9.Hermans R. Staging of laryngeal and hypopharyngeal cancer: value of imaging studies. Eur Radiol. 2006;16(11):2386–2400. doi: 10.1007/s00330-006-0301-7. [DOI] [PubMed] [Google Scholar]
- 10.Becker M, Zbären P, Delavelle J, et al. Neoplastic invasion of the laryngeal cartilage: reassessment of criteria for diagnosis at CT. Radiology. 1997;203(2):521–532. doi: 10.1148/radiology.203.2.9114116. [DOI] [PubMed] [Google Scholar]
- 11.Loveday EJ. Ultrasound of the larynx. Imaging. 2003;15:109–114. doi: 10.1259/img.15.3.150109. [DOI] [Google Scholar]
- 12.Noyek AM, Renouf JH, Sanders DE, Steinhardt M, Zizmor J. The radiologic diagnosis of malignant tumors of the larynx. J Otolaryngol. 1977;6:368–373. [PubMed] [Google Scholar]
- 13.Gritzmann N, Traxler M, Grasl M, Pavelka R. Advanced laryngeal cancer: sonographic assessment. Radiology. 1989;171:171–175. doi: 10.1148/radiology.171.1.2648469. [DOI] [PubMed] [Google Scholar]
- 14.Dhoot NM, Singh S, Choudhury B, et al. Evaluation of hypopharyngeal carcinoma using high-resolution ultrasound: comparison with CT. J Clin Ultrasound. 2014;42:143–149. doi: 10.1002/jcu.22130. [DOI] [PubMed] [Google Scholar]
- 15.Beitler JJ, Muller S, Grist WJ, et al. Prognostic accuracy of computed tomography findings for patients with laryngeal cancer undergoing laryngectomy. J Clin Oncol. 2010;28(14):2318–2322. doi: 10.1200/JCO.2009.24.7544. [DOI] [PubMed] [Google Scholar]
- 16.Xia C-X, Zhu Q, Zhao H-X, Yan F, Li S-L, Zhang S-M (2013) Usefulness of ultrasonography in assessment of laryngeal carcinoma. Br J Radiol 86(1030):343–349 [DOI] [PMC free article] [PubMed]
- 17.Zbären P, Becker M, Läng H. Pretherapeutic staging of laryngeal carcinoma: clinical findings, computed tomography, and magnetic resonance imaging compared with histopathology. Cancer. 1996;77(7):1263–1273. doi: 10.1002/(SICI)1097-0142(19960401)77:7<1263::AID-CNCR6>3.0.CO;2-J. [DOI] [PubMed] [Google Scholar]
- 18.Becker M, Zbären P, Laeng H, Stoupis C, Porcellini B, Vock P. Neoplastic invasion of the laryngeal cartilage: comparison of MR imaging and CT with histopathologic correlation. Radiology. 1995;194(3):661–669. doi: 10.1148/radiology.194.3.7862960. [DOI] [PubMed] [Google Scholar]
- 19.Li B, Bobinski M, Gandour-Edwards R, Farwell DG, Chen AM. Overstaging of cartilage invasion by multidetector CT scan for laryngeal cancer and its potential effect on the use of organ preservation with chemoradiation. Br J Radiol. 2011;84(997):64–69. doi: 10.1259/bjr/66700901. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin. 2011;61:69–90. doi: 10.3322/caac.20107. [DOI] [PubMed] [Google Scholar]
- 21.Chevallier P, Marcy PY, Arens C, Raffaelli C, Padovani B, Bruneton JN. Larynx and hypopharynx. In: Bruneton JN, editor. Applications of sonography in head and neck pathology. 2. Berlin: Springer; 2002. pp. 165–191. [Google Scholar]
- 22.Chevallier P, Padovani B, Marcy P, Chevallier A, Bruneton J. Ultrasonography of the larynx and hypopharynx in adults: normal aspects (in French) J Echographie Med Ultrasound. 1997;18:53–67. [Google Scholar]
- 23.Dhoot NM, Hazarika S, Choudhary B, Kotoki AC, Goswami H, Baruah R (2015) Evaluation of tongue cancer using high-resolution sonography-comparison with magnetic resonance imaging. J Ultrasound Med 34(9):1537–1546. doi:10.7863/ultra.15.14.09001 [DOI] [PubMed]
- 24.Becker M, Zbären P, Casselman JW, Kohler R, Dulguerov P, Becker CD. Neoplastic invasion of laryngeal cartilage: reassessment of criteria for diagnosis at MR imaging. Radiology. 2008;249(2):551–559. doi: 10.1148/radiol.2492072183. [DOI] [PubMed] [Google Scholar]
- 25.Wang CP, Chen TC, Yang TL, Chen CN, Lin CF, Lou PJ, et al. Transcutaneous ultrasound for evaluation of vocal fold movement in patients with thyroid disease. Eur J Radiol. 2012;81:e288–e291. doi: 10.1016/j.ejrad.2011.09.020. [DOI] [PubMed] [Google Scholar]
- 26.Adolphs APJ, Boersma NA, Diemel BDM, Eding JEC, Flokstra FE, Wegner I, Grolman W, Braunius W. A systematic review of computed tomography detection of cartilage invasion in laryngeal carcinoma. Laryngoscope. 2015;125:1650–1655. doi: 10.1002/lary.25145. [DOI] [PubMed] [Google Scholar]