
Figure 3. Repeated Measures Analyses Associating Symptom Severity with Cortical Thickness.
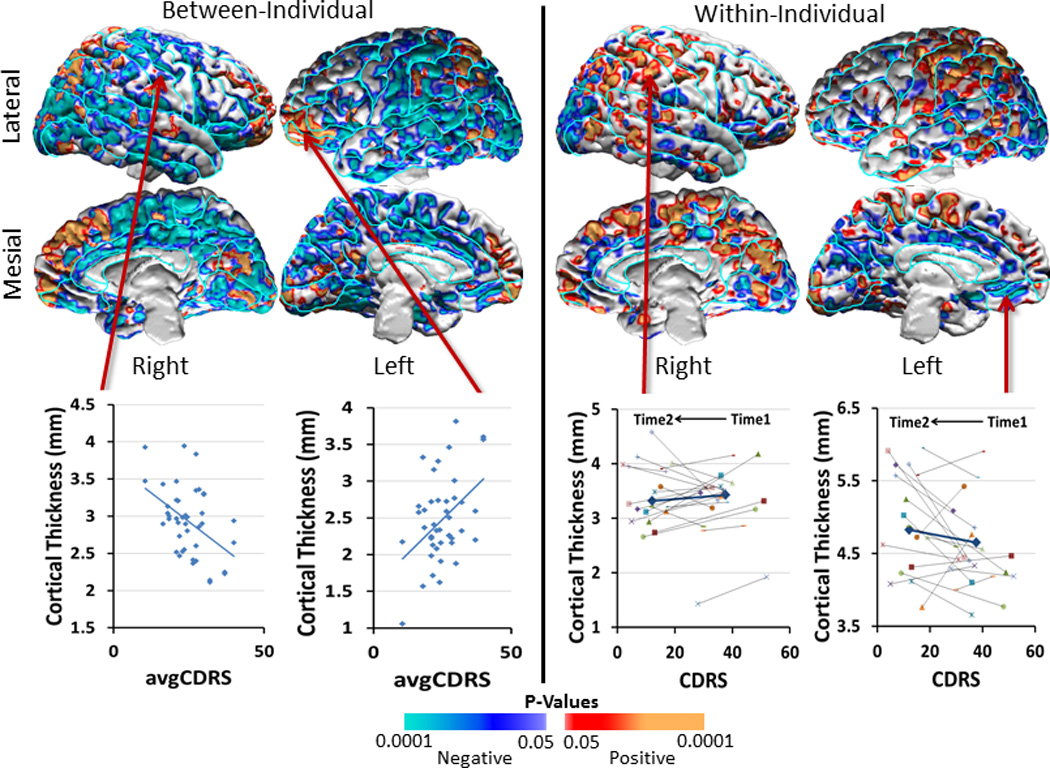
We assessed how cortical thickness in duloxetine-treated patients was associated with symptom severity across individuals, as well as how cortical thickness changed with the change in symptom severity within individuals over time. Symptom severity was measured with the Cornell Dysthymic Rating scale (CDRS). We covaried for age and sex effects and generated scatterplots using age- and sex-adjusted cortical thickness measures. We displayed findings only in voxels where the interaction of treatment-by-time on cortical thickness was statistically significant (Figure 2). Maps of findings across the entire brain are shown in Supplementary Figure 3 of the Supplementary Information.
Left Panel: The cross-sectional, across-individual correlation of cortical thickness with severity showed that thickness correlated inversely with CDRS values, averaged over pretreatment baseline (Time1) and end of trial (Time2), in large expanses of the lateral and mesial surfaces of both hemispheres, especially in regions where the dysthymic patients had thicker cortices than healthy participants at baseline (Figure 1). Scatterplots for representative voxels where inverse correlations were located illustrate that patients with thicker cortices generally had less severe symptoms. In contrast, cortical thickness correlated positively with symptom severity bilaterally in the anterior prefrontal and posterior parietal cortex.
Right Panel: The longitudinal, within-individual, correlation of change in thickness with the change in severity over the course of the trial showed positive associations (indicating that cortical thickness decreased as symptom severity decreased, as shown in orange and red) located bilaterally in the parietal and posterior temporal cortex, and inverse associations (indicating that cortical thickness increased as symptom severity decreased, shown in blue and violet) located bilaterally in the occipital, anterior cingulate, and anterior prefrontal cortex.
Note that the cross-sectional, across-individual maps generally show color codings for correlations that are opposite from those in the longitudinal, within-individual maps: In the left panel, individuals with fewer symptoms had thicker cortices in voxels shown in blue; in the right panel, cortical thickness decreased over the 10-week period of the trial within individuals for whom treatment with antidepressants reduced symptom severity. Thus, the findings in both panels, taken together, suggest that a thicker cortex at baseline is associated with fewer symptoms, likely representing a compensatory, neuroplastic hypertrophy of the cortex. Successful treatment and a decline in symptoms over the course of the trial seems to obviate the need for that compensatory hypertrophy and thereby produces a relative thinning and normalization of the cortical mantle.