

Abstract
Demographic research in sub-Saharan Africa (SSA) has long relied on a blunt urban/rural dichotomy that may obscure important inter-urban fertility and mortality differentials. This paper uses Demographic and Health Survey (DHS) geo-referenced data to look beyond the simple urban/rural division by spatially locating survey clusters along an urban continuum and producing estimates of fertility and child mortality by four city size categories in West Africa. Results show a gradient in urban characteristics and demographic outcomes: the largest cities are the most advantaged and smaller cities least advantaged with respect to access to urban amenities, lower fertility and under-5 survival rates. There is a difference in the patterns of fertility and under-five survival across urban categories, with fertility more linearly associated with city size while the only significant distinction for under-5 survival in urban areas is broadly between the larger and smaller cities. Notably, the small urban “satellite cities” that are adjacent to the largest cities have the most favorable outcomes of all categories. Although smaller urban areas have significantly lower fertility and child mortality than rural areas, in some cases this difference is nearly as large between the smallest and largest urban areas. These results are used to argue for the need to give greater consideration to employing an urban continuum in demographic research.
Keywords: Sub-Saharan Africa, urban continuum, fertility, under-5 mortality, urban/rural dichotomy
INTRODUCTION
Urban dwellers in SSA generally enjoy superior living standards, better access to health services and higher levels of education compared to their rural counterparts (Montgomery, 2009). Cities in SSA have long had a mortality advantage over rural areas, particularly for children, due in large part to the concentration of health resources and infrastructure in the region’s urban areas (Gould 1998; National Research Council, 2003; Bocquier et al., 2011a). Fertility is also substantially lower in urban compared to rural areas throughout the region (Kirk & Pillet, 1998; Shapiro & Tambashe, 2002; White et al., 2008), for reasons related to the higher costs of raising children (Easterlin, 1975) and better access to family planning in cities (Cleland et al., 2006), as well as the more favorable views on smaller family size associated with higher levels of socio-economic development and female education found in urban areas (Cleland & Wilson, 1987). It remains unclear, however, whether the urban advantage for child survival and lower fertility applies uniformly across all areas considered “urban” in SSA.
The uncertainty about intra-urban differences for these health outcomes stems from a reliance on a strict urban/rural dichotomy in research on SSA. This oppositional residential definition categorizes urban and rural areas only in contrast to one another and assumes that characteristics found in one category are absent from the other. Although convenient, this dichotomy implicitly assumes homogeneity within this binary urban/rural classification and, by extension, presumes that urban areas of vastly different size have similar rates of fertility and child mortality.
Previous research on inter-urban health differentials in SSA has indicated that fertility and child mortality rates are not uniform across all urban areas. Most of these studies, however, distinguished only the largest cities (generally the capital cities) from all other urban areas and thus may be capturing specific advantages of capital or primate cities that also tend to be economic and political centers nationally, providing little information on differentials across other urban areas. While women in SSA’s largest cities have been shown to have lower fertility than their counterparts in other urban areas, often by as much as one child per woman (Cohen, 1993; Shapiro & Tambashe, 2002), there appear to be no regional studies that have looked at fertility differentials across other urban areas. Using more detailed urban divisions, two studies on child mortality in SSA found smaller urban areas had worse child survival outcomes than large or medium-sized cities (Brockerhoff & Brennan, 1998; National Research Council, 2003), suggesting a hierarchy for child survival by city size.
While data limitations have long made it difficult to employ a residential continuum in SSA, recent increases in the availability of geo-referenced survey data provide new opportunities to define and incorporate measurements of an urban continuum. Here, I make use of publically available spatial data to produce locally informed estimates of fertility and under-5 mortality by specific urban sub-categories. I match demographic data collected at the administrative level (from household surveys) with data on spatial identifiers (for categorizing survey clusters by city size) by incorporating a geographic information systems (GIS) element that allows for inclusion of a more detailed spectrum of “urban” areas in four distinct urban sub-categories. I focus specifically on West Africa because the sub-region is projected to have the highest rates of urbanization and urban growth within SSA in the coming decades (United Nations, 2012). To the best of my knowledge this is the first demographic analysis which has combined satellite and spatial data with household-survey cluster data to measure and compare inter-urban differences in fertility and child mortality across standardized urban categories.
Failing to account for variation in demographic outcomes across urban areas of different sizes may obscure important differences in fertility and child mortality rates among the diverse and rapidly growing set of settlement areas that fall under the singular “urban” category used in most demographic research. Disparities identified in health outcomes between urban and rural areas have been influential in allocating resources aimed at improving child survival and access to voluntary family planning; if there is substantial inter-urban variation in fertility and child mortality outcomes, then similar consideration should be given to program and policy approaches for urban areas of different size. In this study, I aim to determine whether fertility and child mortality rates across urban areas in West Africa differ significantly enough to justify a call for greater use of an urban continuum in demographic research in the region – or whether, conversely, urban areas of different sizes have fertility and mortality rates similar enough to justify continued reliance on the urban/rural dichotomy.
DATA
In order to link local demographic data collected from household surveys to standardized city size categories across West Africa, I combine data from three sources. First, I take population estimates of urban areas from country censuses. I then delineate the boundaries of these urban areas using the Global Urban-Rural Mapping Project (GRUMP). Next, I use geo-locating survey clusters from the DHS within these urban extents to categorize the survey clusters by city size category. Last, I calculate local estimates of fertility and child mortality rates and then aggregate them by city size category at the regional level.
I use the most recent data from the eight West African countries with a Standard DHS that provided GPS cluster coordinates and had a census conducted five years before or after the survey: Benin, Burkina Faso, Cote d’Ivoire, Ghana, Guinea, Mali, Niger and Senegal (Table 1). This sample is limited to countries with a census within five years of a DHS because rapid urban growth in the region could result in substantial changes to city populations over a short period of time, particularly for smaller urban settlements. According to UN population estimates, the countries account for 40% of West Africa’s population; when Nigeria (the most populous country in Africa) is removed from the regional population estimate, they then represent 84% of the total.
Table 1.
DHS surveys and country census data included in the analysis
| DHS
|
Nearest census year | Census population count (′000) | |
|---|---|---|---|
| Country | Year | ||
| Benin | 2001 | 2002 | 6,770 |
| Burkina Faso | 2010 | 2006 | 15,225 |
| Côte d’Ivoire | 1998 | 1998 | 15,366 |
| Ghana | 2008 | 2010 | 24,659 |
| Guinea | 1999 | 1996 | 7,156 |
| Mali | 2006 | 2009 | 14,529 |
| Niger | 1998 | 2001 | 11,060 |
| Senegal | 2011 | 2010 | 16,509 |
SOURCE: Demographic and Health Surveys; Individual country census counts accessed from www.citypopulation.de.
Census Data
Population estimates of urban areas are derived from individual country censuses. This data is accessed from the citypopulation.de website, which compiles data on national and urban populations for publicly available censuses and lists population counts for all areas classified as urban (Brinkhoff, 2014). In this analysis, all urban population counts from census data are for the city proper (administrative boundaries) because estimates for urban agglomerations (which may include adjacent cities or towns) are specified for some but not all countries.
Demographic and Health Surveys (DHS)
Data on local levels of fertility, child mortality and socio-demographic characteristics come from the DHS. The DHS collects nationally representative data in low- and middle-income countries through household sample surveys designed to measure health, population, and socioeconomic indicators, with a specific focus on maternal and child health (Rutstein & Rojas, 2006). Fertility and child mortality rates can be directly calculated from birth histories in the DHS that provide data on the month and year of birth, parity, sex, and survivorship status of each child ever born to a respondent.
The DHS also includes information on three variables that measure access to urban amenities and can serve as a functional measure of urbanness: household electrification, access to an improved source of drinking water and access to improved sanitation (toilet facilities) (Dorélien et al., 2013). These amenities, which tend to be concentrated in urban areas in SSA, have been shown to be positively correlated with child survival (Mosley & Chen, 1984; Wang, 2002; Fink et al., 2011). Household electrification is a binary outcome for whether electricity is available in a respondent’s household. Improved water source and sanitation categories are based on definitions from the WHO and UNICEF Joint Monitoring Program for Water Supply and Sanitation (WHO/UNICEF JMP, 2010).1
In the DHS, each survey cluster is identified as either “urban” or “rural” (v025) according to definitions from each country’s national statistics office. Some DHS also include a more detailed residence variable (v026) which further classifies cluster locations as “capital/large city”, “small city”, “town”, or “countryside”. Relying on the v026 variable to create cross-country sub-categories of urban settlements, however, is problematic because 1) these classifications are generally based on interviewer judgement, and not official population counts, and may vary across countries, 2) the variable does not identify specific cities, making it impossible to determine to which urban area a cluster corresponds when there are several within a region, and 3) the number of categories for this variable is not standardized across surveys, with some including three categories and others four. Thus, while v026 provides a loose division of urban areas according to size, it is not consistent enough to be systematically incorporated in most cross-country comparisons, which may explain in part why most regional or multi-country studies divide residence using only the urban/rural dichotomy.
The majority of DHS, however, now include geo-referencing information by providing the longitude and latitude coordinates for all clusters that allows for the visual identification of their locations. The accuracy of these cluster locations is estimated to be within 15 meters (ICF International, 2013), but in order to guarantee respondent confidentiality urban clusters are displaced up to two kilometers and rural clusters up to five kilometers in the publically available datasets (Burgert et al., 2013). As a result, mapped cluster placements are close to but not the exact locations of the actual survey clusters.
The Global Rural-Urban Mapping Project (GRUMP)
I use the GRUMP urban extents database to spatially identify urban boundaries and to subsequently match survey clusters to specific cities and urban settlements. GRUMP is a global database that approximates the extent of urban areas by combining nighttime lights satellite data with administrative information on population sizes of settlement areas, allowing for a more standard identification of urban extents globally than do comparisons of individual country-level administrative data (Balk et al., 2005). GRUMP initially identifies urban areas by their night-time lights “footprint” using the National Oceanic and Atmospheric Administration’s (NOAA) 1994–95 stable city lights dataset to calculate urban areas as a propensity of the lights-based extents, then matches these areas to information on city name and population size from national statistics offices and external sources (GRUMP, 2014). The ultimate assignment of urban extents with GRUMP involves several levels of cross-validating data from local administrative sources on population and settlement sites with satellite data, resulting in what has been characterized as crude but largely accurate representations of urban extents associated with human settlements (Balk et al., 2005).
Electrification is often used to identify urban settlements in developing countries because it is highly concentrated in cities (Doll & Pachauri, 2010) and the economic activity generally associated with urban areas is strongly correlated with nighttime lights (Henderson et al., 2012). While electricity is not absent from all rural areas, where present it is often not strong enough to be detected by the satellite imagery of nighttime lights (Dorélien et al., 2013). As a result, in less developed regions the NOAA nighttime lights data sometimes does not detect known smaller cities or towns, and in these instances GRUMP estimates the urban extents using alternative means (for details see Balk et al. 2009; Dorélien et al. 2013). These imputed urban areas are designated with fictive lights in the shape of a circle to differentiate them from the satellite data polygons that represent areas captured by the nighttime stable lights.
There are several advantages to using the GRUMP-identified urban extents, rather than national administrative data, for identifying urban settlements and for placing DHS survey clusters along an urban continuum. First, official administrative sources of urban areas may rely on outdated definitions and do not account for urban growth and expansion. For example, Dorélien et al. (2013) found that in SSA GRUMP identified as urban many clusters designated as rural in the DHS and that clusters within the GRUMP extents were likely to have urban characteristics, suggesting that many administrative data sources in SSA do not accurately capture population change. Second, combining DHS clusters with GRUMP data can help identify clusters that appear to be miscoded, as when a rural cluster clearly falls within a group of urban clusters in a major GRUMP urban extent. Finally, matching DHS clusters to the GRUMP-identified urban extents facilitates a placement of clusters along a continuum of urbanness that is not possible by relying on administrative data (Dorélien et al. 2013) through the identification of “peri-urban” clusters that are considered rural in the DHS but fall within a broader urban extent of a nearby city as identified by GRUMP.
The GRUMP dataset is not without its limitations (Balk 2009), two of which are relevant here. First, GRUMP was developed using the NOAA stable city-lights dataset from 1994–95 and thus does not capture areas that became electrified after this period, although this is partially compensated here by the broad matching of GRUMP urban extents with more recent data from the NOAA nighttime lights satellite data.2 Second, the GRUMP dataset has been shown to overestimate urban areas as a result of “overglow” from its satellite readings (McGranahan et al. 2007; Elvidge et al. 2004). While other nighttime lights databases, for example the VIIRS (Visible Infrared Imaging Radiometer Suite) lights or MODIS urban extents, have higher resolution and thus more accurate readings of urban lights extents, they do not provide direct links to geographic identifiers for urban areas. Thus the ease of matching the GRUMP lights to specific urban areas, due to the cross-validation with administrative and population data in the creation of the database, makes it preferable over these other sources for use both in this analysis and in future work that seeks to link urban areas –particularly smaller settlements– to nighttime lights satellite data.
City class categories
There is no international or standardized definition of urban and rural, and consequently each country determines how to classify settlements as urban or rural.3 Here, in order to create a systematic and regionally consistent measure of urban size, I create four standard categories of cities (Classes 1–4) based on census population counts. The largest cities (Class 1) have populations over 1 million. The smallest cities (Class 4) have populations less than 50,000 and are designated by the national statistics office (and hence the DHS) in their respective countries as urban.4 Class 2 cities have populations between 150,000 to 1 million, and Class 3 from 50,000 to150,000 (Table 3). The cutoff of 150,000 between Class 2 and Class 3 cities was chosen because a higher threshold resulted in a very small number of cities and clusters in Class 2 (as West Africa has few secondary cities) and using a lower bound for Class 3 (50,000–100,000) resulted in an uneven distribution of DHS clusters across the analysis countries. An additional cut-off of 500,000 between 100,000 and 1 million has been used in research on child mortality across different world regions (National Research Council, 2003), but this threshold was again problematic in West Africa because so few cities fall into this category.5
Table 3.
Cities and DHS cluster distribution per class size
| Urban Classification | Population size | Cities | Number of DHS clusters | Proportion of urban clusters |
|---|---|---|---|---|
| Class 1 | > 1million | 7 | 297 | 28% |
| Class 2 | 150,000 – 1 million | 23 | 174 | 16% |
| Class 3 | 50,000 – 150,000 | 70 | 198 | 18% |
| Class 4 | < 50,000 | 317 | 406 | 38% |
|
| ||||
| Total | 416 | 1,075 | 100% | |
Last, I create a separate fifth category of urban areas that I designate “satellite cities”: cities that fall into Classes 2, 3 or 4 (and designated in their respective DHS as “small cities” or “towns”) and are adjacent to a Class 1 city. Although considered separate administrative settlements with distinct census population counts, these smaller cities may be more akin to suburbs or extensions of their neighboring large cities because they fall within the contiguous territory of urban density levels (here GRUMP nighttime lights serve as a proxy for population density) and would generally be considered part of the larger “urban agglomeration” (United Nations, 2012). Only a small proportion of all urban clusters fit this category (in Benin, Cote d’Ivoire, Ghana, Mali and Senegal) (Table 4), though this may reflect DHS sampling rather than actual population distribution. The standard analysis here is run for the first four city class categories, with this fifth segmented “satellite city” category included only where indicated.
Table 4.
Reclassified clusters: “satellite city” (Class 5) clusters and rural DHS clusters that fall within GRUMP urban extents
| Reclassification | DHS clusters (n) | Proportion of total urban clusters |
|---|---|---|
| Reclassified urban “satellite” clusters: | ||
| City Class 1 | – | – |
| City Class 2 | 5 | 0.47 % |
| City Class 3 | 16 | 1.49 % |
| City Class 4 | – | – |
|
|
||
| Total Class 5 “satellite” clusters | 21 | 1.96 % |
|
| ||
| Reclassified “peri-urban” rural clusters: | ||
| City Class 1, 2 & 3 | 32 | 1.93 % |
| City Class 4 | 19 | 1.15 % |
| GRUMP Imputed circles | 20 | 1.21 % |
|
|
||
| Total peri-urban clusters | 71 | 4.29 % |
Survey cluster mapping
To link each cluster to a specific urban area, I first spatially located all clusters identified as urban by their respective DHS using ArcMap 10.1. I then added the GRUMP urban extents data to this base so that clusters could be matched to specific urban areas with populations greater than 50,000. Designation of clusters in the Class 4 category (with populations of fewer than 50,000), however, is less precise because it relies on DHS classifications rather than geo-spatial matching, due to the challenges of identifying the exact location of these smallest urban areas, particularly those that have emerged since 1995 and would not be captured by GRUMP. Consequently, not all urban areas that fall under Class 4 can be fully verified, and there is a leap of faith in assuming that the smaller “urban” areas are accurately defined by their respective DHS urban/rural designations.
The Class 5 satellite city category consists of clusters that are adjacent to a Class 1 city but that fall under a separate administrative area. “Adjacent” is defined here as located within 20 kilometers of the administrative boundary of the Class 1 city and within the contiguous GRUMP nighttime lights urban extent. By layering the GRUMP database over administrative boundaries (as identified by GRUMP and by shapefiles based on national administrative data), city-specific population estimates can be matched to separate urban areas where multiple cities or towns fall under a single GRUMP nighttime lights spatial extent. Map 1 illustrates this for clusters from the Ghana 2008 DHS that fall within Class 5 satellite cities.
Map 1.
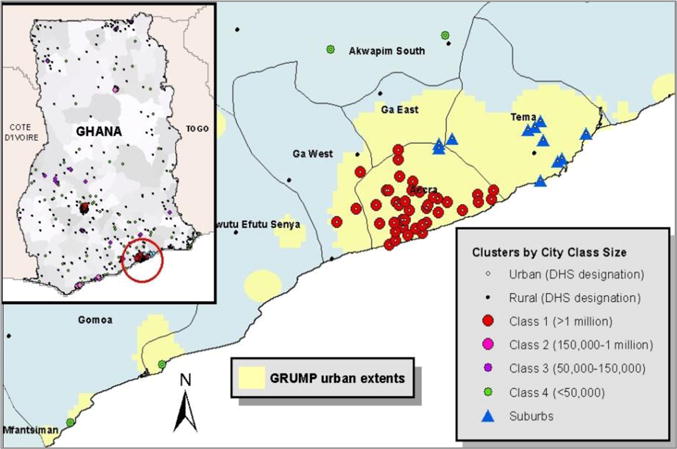
“Satellite city” category mapping for Ghana clusters, DHS 2008
Finally, I designate as “peri-urban” clusters that are identified as rural in the DHS but fall within GRUMP identified urban extents. Map 2 illustrates this process for the interior of Senegal. These peri-urban categories are analyzed separately to determine whether a) they have urban characteristics and demographic outcomes more similar to urban or rural areas, and b) if there is a gradation in urban fertility and child mortality rates in the peri-urban areas that is similar to their associated city class categories. These reclassified rural clusters are divided into three categories: 1) clusters associated with Class 1, 2 and 3 cities (combined into one category because of the small number of clusters that fall under each city class); 2) clusters within Class 4 cities (the category that relies on each individual country’s definition of a lower threshold of urban); and 3) rural clusters that fall within the GRUMP imputed circles, as these circles represent a different measurement of urban (imputed rather than identified by electrification). The displacement of up to 5 kilometers for rural clusters in DHS means some clusters that are truly rural will be displaced into urban light extents, while some rural clusters that actually fall within these extents will be displaced outside of them. For categorization purposes, however, I assume that clusters are accurately matched and that the noise from the displacement will be washed out.6
Map 2.
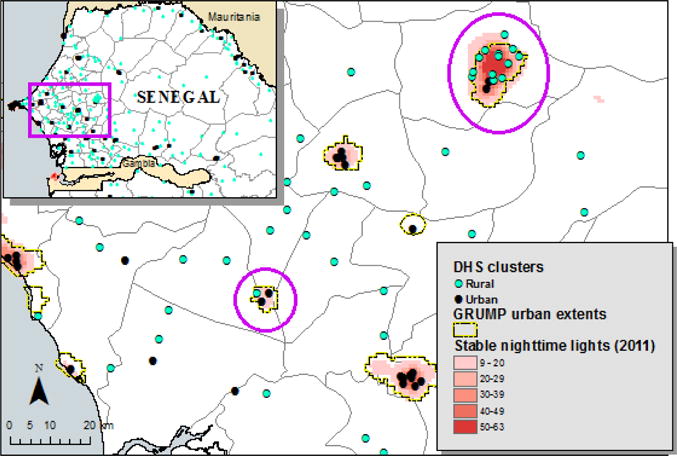
Rural clusters re-categorized as “peri-urban” for Senegal, DHS 2011
METHODS
Descriptive Statistics
The descriptive overview includes comparisons of weighted averages of three of the main indicators of access to urban amenities (the proportion of households with electrification, access to clean water, and improved sanitation) that are captured by DHS surveys.
Fertility
Total fertility rates (TFR) are calculated first for all urban and rural areas, then separately by city class size and peri-urban categories.7 TFR is estimated using the tfr2 Stata module (Schoumaker, 2013) that computes both age-specific fertility rates and TFR, as well as their standard errors. In this analysis, TFR is calculated for the five years prior to the survey, rather than the standard three years, to provide a more accurate measurement of fertility for the smaller sample size of women in the “satellite city” category. Unlike the estimates of under-5 mortality (see below), a woman’s recent migration status is not taken into account for TFR calculations, as these are estimates of lifetime fertility and thus it is the total number of births, and not the location in which they occurred, that is of interest.
Under-5 mortality
Under-5 mortality rates (more specifically the probability of a child dying before reaching his or her fifth birthday) are calculated here using Kaplan-Meier survival curves, which provide a nonparametric estimate of the survivor function S(t), the probability of survival past time t (Cleves et al., 2010). All children born within the ten years preceding the survey are included and considered at risk of death until age five, and right-censored when they reach age five or at the time of death if they die before their fifth birthday. Employing the Kaplan-Meier method prevents misattribution of time at risk or death when a child has moved (or when a mother has moved after the death of a child)8 by permitting both right and left censoring; this allows for attribution of a child’s exposure time or death to a prior place of residence rather than assuming that all exposure and deaths occurred in the place in which the survey was conducted (Bocquier et al., 2011a). The DHS does not provide enough specific information on previous place of residence to attribute pre-migration exposure to specific city class size, so children whose mothers changed residence are left censored after the last move into the observation period for the city category in which they were living at the time of the survey, eliminating the inclusion of pre-migration time at risk or deaths into the city class-specific calculations. As Stata cannot produce standard errors or 95% confidence intervals for the survival probabilities with complex weights, I use the logrank test of equality to determine whether under-5 survival probabilities in specific residence areas are significantly different from one another and note these comparisons directly in the text.
I perform all analysis at the regional level, not for individual countries, for reasons that are both theoretical and practical. Theoretically, creating these city class categories allows for systematic and consistent measures of city size needed to examine dominant patterns and produce generalizable findings of fertility and mortality differentials across West Africa. More practically, small sample sizes for city-specific estimates often render estimates at the individual country level impractical or, in many cases, impossible. For example, smaller urban areas often have only one survey cluster, while many of the largest urban areas have only a handful of clusters – both of which are generally insufficient to make meaningful demographic estimates. In all steps of the analysis, the data is pooled at the regional level and includes both complex survey weights and population size weights in order to account for the DHS multistage sampling design and to produce results that are representative of the population at the regional level. TFR and under-5 survival models also control for clustering at the primary sampling stage to produce adjusted standard errors that account for within-cluster correlations.
RESULTS
Urban residents are more likely than those in rural areas to have electrification, access to clean water and improved sanitation (Table 5). Electrification and improved sanitation show the largest urban/rural differences, with over 70% of urban dwellers overall having access to these amenities compared to only a fifth of those in rural areas. Within urban areas, proportional access to these urban amenities declines as city size decreases. Household electrification and improved toilet facilities show the largest inter-urban differences while access to improved water varies the least across city class categories. This may reflect the fact that electricity and sanitation are largely determined by infrastructure, whereas potable water can be accessed at the neighborhood level (e.g. a local pump that serves many families) or purchased. Notably, the proportion of households with access to all three urban amenities in Class 4 cities is still well above the rural averages, highlighting a distinct difference between even the smallest urban areas and those designated rural.
Table 5.
Mean % of households with household electricity, access to improved drinking water and improved sanitation, DHS surveys 1998–2011
| Location | Electrification (%) | Improved water (%) | Improved sanitation (%) |
|---|---|---|---|
| Overall | 37.6 | 63.7 | 39.0 |
| Urban/Rural (DHS designation) | |||
| Urban | 74.4 | 82.2 | 69.8 |
| Rural | 15.2 | 51.7 | 20.2 |
| City Class Categories (1–4) | |||
| Class 1 (> 1million) | 85.9 | 85.7 | 83.6 |
| Class 2 (150,000 – 1 million) | 78.3 | 81.0 | 71.2 |
| Class 3 (50,000 – 150,000) | 64.2 | 82.4 | 56.6 |
| Class 4 (< 50,000) | 60.4 | 77.1 | 55.5 |
| City Class urban categories with “satellite” cities segmented | |||
| Class 1 (> 1million) | 85.9 | 85.7 | 83.5 |
| Class 2 (150,000 – 1 million) | 77.0 | 79.7 | 69.1 |
| Class 3 (50,000 – 150,000) | 59.7 | 79.9 | 52.6 |
| Class 4 (< 50,000) | 60.4 | 77.1 | 55.5 |
| Class 5 (Class 1 satellite cities) | 94.5 | 97.7 | 87.7 |
| Re-categorized rural clusters | |||
| Peri-urban (Class 1, 2 & 3) | 72.7 | 96.1 | 76.1 |
| Peri-urban (Class 4) | 22.6 | 59.2 | 26.4 |
| Peri-urban (imputed circles) | 2.4 | 23.2 | 7.8 |
NOTES: Results were calculated for the pooled sample by residential type and were weighted at the country level to account for the multistage sampling design and country population at the regional level.
SOURCE: DHS data; author’s calculations.
There is also a gradient in access to urban amenities among the three “peri-urban” categories, as clusters associated with medium and large cities have proportional access to urban amenities similar to these urban areas. Interestingly, access to improved water for this group appears to be nearly universal (96%) and is higher than any other urban category. Peri-urban clusters that fall within Class 4 city extents have access to urban amenities that is lower than in the smallest urban areas but greater than the rural average. Peri-urban clusters that fall within GRUMP imputed circles have urban characteristics below even the rural average.
Satellite city clusters, those adjacent to the largest urban areas, have higher proportional access to urban amenities than any other city class category, including the Class 1 cities to which they are adjacent. Segmenting clusters from these satellite cities results in slight changes for Class 2 and 3 categories (from which the satellite cities are removed): Class 3 and 4 cities now have nearly equal access to all three amenities, and Class 3 even drops below Class 4 for access to improved water.
Fertility shows a stark urban/rural contrast: women in rural areas have a TFR of 6.47 compared to 4.09 for all urban areas combined. Within urban areas, there is a clear fertility gradation across the city class categories (Table 6), with a difference of over half a child between the Class 1 and 2 cities (0.63) and again between Class 2 and 3 cities (0.51). The TFR differentials are much smaller, however, between Class 3 and 4 cities (0.22). This gradient in fertility mirrors the slope found for urban characteristics across city categories: Class 1 cities are the most advantaged, Class 2 cities slightly less advantaged but still much more favorable than Class 3, with little difference between Class 3 and 4 cities. When segmented, Class 5 satellite cities have the lowest fertility of any urban area (including Class 1 cities), though the variance also is much higher. Removing the satellite city clusters from Classes 2 and 3 increases the TFR slightly for both categories (from 4.07 to 4.11 for and from 4.58 to 4.83, respectively), and Class 3 and 4 cities now have adjusted TFRs that are nearly identical.
Table 6.
Total Fertility Rate (TFR) and under-5 survival probabilities by residence type, DHS surveys 1998–2011
| Location |
Fertility
|
Child mortality
|
|||
|---|---|---|---|---|---|
| TFR | SE | n women | Under-5 mortality | n children | |
| Overall | 5.58 | 0.024 | 75,612 | 0.166 | 237,874 |
| Urban/Rural (DHS designation) | |||||
| Urban | 4.09 | 0.034 | 27,919 | 0.113 | 66,236 |
| Rural | 6.47 | 0.032 | 47,693 | 0.186 | 171,638 |
| City Class 1–4 urban categories | |||||
| Class 1 (> 1 million) | 3.44 | 0.059 | 7,625 | 0.096 | 15,408 |
| Class 2 (150,000 – 1 million) | 4.07 | 0.081 | 4,987 | 0.097 | 10,504 |
| Class 3 (50,000 – 150,000) | 4.58 | 0.087 | 4,926 | 0.131 | 12,604 |
| Class 4 (< 50,000) | 4.80 | 0.060 | 10,381 | 0.127 | 27,720 |
| City Class urban categories with “satellite” cities segmented | |||||
| Class 1 (> 1 million) | 3.44 | 0.059 | 7,625 | 0.096 | 15,408 |
| Class 2 (150,000 – 1 million) | 4.11 | 0.084 | 4,840 | 0.100 | 10,223 |
| Class 3 (50,000 – 150,000) | 4.83 | 0.091 | 4,613 | 0.137 | 12,032 |
| Class 4 (< 50,000) | 4.80 | 0.060 | 10,381 | 0.127 | 27,720 |
| Class 5 (“satellite cities”) | 3.26 | 0.246 | 460 | 0.058 | 853 |
| Re-categorized rural clusters | |||||
| Peri-urban (Class 1, 2 & 3) | 4.27 | 0.229 | 998 | 0.133 | 2,422 |
| Peri-urban (Class 4) | 5.80 | 0.417 | 421 | 0.206 | 1,445 |
| Peri-urban (imputed circles) | 7.45 | 0.389 | 582 | 0.254 | 1,841 |
NOTES: Results were calculated for the pooled sample by residential type and were weighted at the country level to account for the multistage sampling design and by country population at the regional level.
SOURCE: DHS data; author’s calculations.
Peri-urban clusters associated with medium and larger cities have a TFR (4.27) that falls in the middle of the overall urban average, and peri-urban clusters associated with Class 4 polygon extents have TFR (5.80) that is lower than the rural average (6.47) but still substantially higher than the Class 4 average (4.09). Surprisingly, rural clusters located within GRUMP imputed circles have TFR that far surpasses even the rural average, at 7.45, though this seems to be highly influenced by two groupings of clusters from Niger with TFRs that are exceptionally high (between 8 and 10 children per woman), even for Niger.
Under-5 survival probabilities, like TFR, show significant differences between urban and rural dwellers (Table 10): children in urban areas are 7% more likely to reach age five than their rural counterparts (significant at p<.01 for the log-rank test of equality). In contrast to fertility, however, under-5 survival probabilities are nearly identical for the two largest city categories, and the difference between them is not statistically significant (p>.05). Likewise, survival probabilities are similar and not significantly different (p>.05) between Class 3 and 4 cities. The difference in survival probabilities between combined Class 1 and 2 compared to combined Class 3 and 4 cities, however, is significant (p<.001). The only significant distinction for under-5 survival in urban areas appears to be that between larger and smaller cities.
For child survival, the segmented Class 5 satellite cities again have the most favorable outcome of any urban category. Children living in the satellite cities are nearly 4% more likely to live to age 5 than those living in Class 1 or 2 cities (p<.05). Similar to the TFR pattern, removing the satellite city clusters from the Class 2 and 3 categories lowers survival probabilities slightly for both these categories.
Kaplan-Meier survival curves illustrate these patterns for under-5 survival, showing that survival probabilities are nearly identical for Class 1 and 2 cities, and are very similar again for Class 3 and 4 cities. The survival curves are clearly higher in the two larger compared to two smaller city categories, and are consistently highest for all five years in the Class 5 satellite cities.
DISCUSSION
The gradient in fertility and child mortality across urban areas of different size in West Africa mirrors patterns in proportional access to the urban amenities that approximate “urbanness”: the more “urban” the city class category, the lower the rates of fertility and child mortality. Employing a more detailed urban continuum reveals an absolute difference in TFR between the smallest and largest cities (1.36) that is nearly the same as between the smallest cities and the rural average (1.67). While inter-urban differences in under-5 mortality are not as dramatic as those between urban and rural areas, children in the largest two city categories are still approximately 4% more likely to survive to age 5 than their counterparts in smaller cities (p<.001).
The slightly different patterns for the inter-urban gradient between TFR and under-5 mortality, however, suggest a difference in the association of these two outcomes with urban characteristics. While each step up in city class size is associated with lower TFR, the probability of surviving to age five is very similar for Class 1 and 2 cities, and nearly the same between Class 3 and 4 cities. Child mortality rates between the two categories of larger urban areas (Classes 1 and 2) are practically indistinguishable, suggesting that the largest city advantage previously found in the SSA setting (Brockerhoff & Brennan, 1998; National Research Council, 2003) also extends to medium-large cities. Likewise, the smaller city disadvantage seems to apply evenly to both medium-small and the smallest urban areas in the West African context. This small city disadvantage may be cause for concern, as smaller cities in West Africa are projected to have the greatest proportional urban growth in the coming decades but will likely have fewer resources for meeting the needs of growing populations as they tend to be relatively underserved by government services compared to bigger cities (National Research Council, 2003; Montgomery, 2009; UN-Habitat, 2010). Although they lag behind larger cities, the smallest urban areas still have more favorable fertility and child mortality outcomes compared with rural areas. This is most notable for under-5 mortality, for which the absolute difference between rural areas and smaller cities (0.059, or approximately a 6% greater chance of reaching age five in small cities) is nearly twice that between smallest and largest cities (0.031, or approximately a 3% greater chance of reaching age five in the largest cities).
Class 5 cities not only appear extremely urban in terms of access to all urban amenities, they also exhibit extremely “urban” demographic behavior, with the lowest TFR and under-5 mortality of any urban category. The positive profiles found for these satellite cities runs counter to much of the conventional wisdom on urban SSA that often characterizes most surrounding areas of major cities as disadvantaged informal settlements, and suggest instead that there may be substantial variation in the profiles of areas surrounding largest cities. Where possible, future research on urban areas in SSA should specifically segment these outlying satellite cities, as they appear to be distinct from the major urban areas to which they are adjacent but may also make up an important part of the fabric of the region’s major urban agglomerations.
For the outcomes measured here, the “peri-urban” clusters (designated in the DHS as rural but which fall within the GRUMP urban extents) are perhaps more aptly described as “semi-urban”: they appear neither fully urban nor fully rural but rather a combination of both. This is particularly true for peri-urban clusters associated with GRUMP nighttime lights polygons, which have urban characteristics and demographic outcomes that fall between those found in rural areas and those in the urban areas with which they are associated. Peri-urban clusters spatially located within GRUMP imputed circles, however, have urban characteristics below even the rural average and TFR and child mortality rates higher than the rural average. This indicates that GRUMP urban extents that are imputed do not capture areas with urban characteristics as well as those identified by nighttime lights polygons, and seems to add to the evidence that electricity in SSA is strongly correlated with urbanness.
As most DHS surveys now include geo-referenced data for survey clusters, combining GRUMP satellite data with DHS spatial data allows for the incorporation of a more detailed urban continuum in demographic research. For analysis that cannot incorporate GIS aspects directly, the DHS should more systematically include variable v026 with four standard categories. Although it represents a less precise or standardized division of urban areas, v026 nonetheless provides a basic distinction among the largest, medium and smaller urban areas, allowing for an easy incorporation of an urban hierarchy in studies using DHS data. A more systematic inclusion of v026 in all DHS may also help determine whether this variable can be accurately used for cross-country comparisons.
This study has several limitations that could be addressed in future research and data collection. First, the city class categories here are not precise measurements of thresholds at which fertility or mortality rates change but are instead general divisions meant to broadly identify overall patterns in urban characteristics and demographic outcomes by city size. Determining whether there are more accurate thresholds for these divisions will require further exploration. Second, the GRUMP dataset uses satellite imagery from 1994–95 and thus does not capture any areas with new or increased electrification since that time. Here, NOAA nighttime lights dataset from later years were compared to the GRUMP urban extents data in an attempt to identify major changes, but it would be preferable to have a systematic update of the GRUMP urban extents using more recent satellite data. Third, the low fertility and child mortality rates found in satellite cities could be a reflection of biased sampling. Other research has pointed out that the DHS may fail to sample the poorest parts of urban areas (see, e.g., UN-Habitat 2003a; Gunther & Harttgen 2012; Olack et al. 2011), and the extremely favorable fertility and child mortality of the satellite cities found here could be a reflection of sampling error if wealthier outlying areas were sampled. Larger survey samples from these specific areas are needed to make meaningful inferences about these localities; until then, results here related to these satellite cities should be interpreted with caution. Last, as this analysis seeks to identify broad patterns across urban areas, it does not account for differences in population composition or control for known covariates of fertility and child mortality, nor does it explore to how these variables influence overall urban fertility and mortality rates. Some urban sub-populations are at greater risks for under-5 mortality (Fink et al., 2014; Gunther and Harttgen, 2012; National Research Council, 2003), and future research could examine the distribution of the known correlates of fertility and child mortality across urban areas of different size to better understand how they influence the aggregate averages.
CONCLUSION
The continued reliance on a simple urban/rural dichotomy in demographic research conceals inter-urban differences that can as be as substantial as those between urban and rural areas. Results from combining survey and GIS data to create an urban continuum show a clear gradation in fertility and child mortality rates associated with city size: fertility and child mortality are lowest in the biggest cities and the highest in smaller cities. There are two notable exceptions to this pattern. First, while TFR to increases fairly linearly across urban size categories, under-5 mortality is nearly identical in Class 1 and 2 cities and drops substantially for Class 3 and 4 cities, which also have similar rates. Second, when the smaller “satellite cities” adjacent to the largest cities are segmented from their original city class categories, they have the lowest fertility and under-5 mortality rates of any urban category, and their separation results in the Class 3 cities (with population of 50,000–100,000) having the least favorable fertility and mortality rates; their fertility and child mortality rates are slightly higher than those in the smallest cities (<50,000), although the difference is not statistically significant. Leveraging geo-referenced data also reveals differences among rural clusters based on their location within GRUMP-identified urban areas: clusters that are designated by the DHS as rural but which fall within the GRUMP designated urban extents generally have fertility and child mortality rates that lie between those of the urban areas with which they are associated and other rural areas.
Persistent use of the strict urban/rural division in demographic research may also obscure important interrelationships between the ongoing process of urbanization and declines in fertility and child mortality in West Africa. Findings here suggest it would be a mistake for demographic research in SSA to continue to consider only urban/rural differences in fertility and child mortality. Demographers should instead capitalize on the growing availability of spatial data in the DHS to move away from the convenient but simplistic urban/rural dichotomy and towards an increased implementation of an urban continuum.
Graph 1.
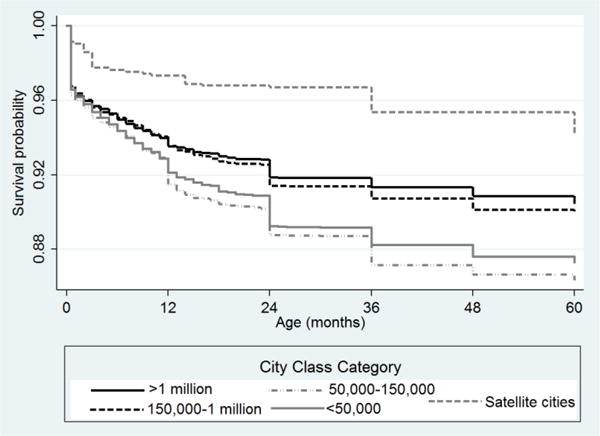
Kaplan-Meier survival curves to age 5 by city class category
Source: Demographic and Health Surveys for Benin, Burkina Faso, Côte d’Ivoire, Ghana, Guinea, Mali, Niger and Senegal.
Table 2.
Description of data sources in the analysis
| Data Source | Data | Use |
|---|---|---|
| Individual Country Censuses | Urban area populations | Classifying urban areas by population size |
| Global Urban-Rural Mapping Project (GRUMP) | Global urban extent boundaries | Mapping and matching DHS clusters to urban areas |
| Demographic and Health Surveys (DHS) | Individual demographic and socio-economic variables | Calculating household characteristics, fertility rates and child mortality rates |
Acknowledgments
This research received support from the Population Research Training grant (NIH T32 HD007242), from the National Institutes of Health’s (NIH)’s Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD), and from the Demography of Aging grant (NIH T32 AG000177) from NIH’s National Institute on Aging (NIA) awarded to the Population Studies Center at the University of Pennsylvania. Special thanks to the City University of New York’s Institute for Demographic Research (CIDR) for additional institutional support and in particular to Deborah Balk for her suggestions during the formative stages of this project.
Footnotes
A household is considered to have access to improved water if its primary source of drinking water comes from a private or public tap, a protected well or spring, or rainwater. Improved sanitation includes a private or shared flush toilet or an improved latrine.
As all of the DHS surveys in this analysis were carried out after 1995, I compared the NOAA nighttime lights dataset from the same year each respective DHS was carried out with the GRUMP urban extents data to determine whether discernable new areas of electrification were visible. As the correspondence between GRUMP and the stable nighttime lights time-series was generally high, only the GRUMP extents are used in the remainder of the analysis. More detailed country-level analysis, however, should consider closer analysis of recent NOAA nighttime lights data with GRUMP. I do not use the newer lights data because, as with VIIRS, they are not linked to location by name.
The lower bound of “urban” is difficult to account for, as it varies by country: for example, in Benin urban areas are settlements with more than 10,000 inhabitants, in Ghana they are localities with more than 5,000, and in Burkina Faso settlements with more than 4,000 are considered urban.
For the countries included in this analysis, only three cities have populations between 500,000 and 1 million (Cotonou in Benin, Niamey in Niger and Touba Mosque in Senegal), although two more come close with populations of just over 400,000 (Bobo Diaoulasso in Burkina Faso and Bouake in Cote d’Ivoire).
This is true for calculating means but not variances, which results in conservative estimates for differences between the City Class categories, suggesting the real differences may be higher than those computed here.
The majority of children under 5 in SSA live with their mothers so any potential bias from separate mother-child residence is believed to be small (Bocquier et al., 2011a).
References
- Allison PD. Using panel-data to estimate the effects of events. Sociological Methods & Research. 1994;23(2):174–199. [Google Scholar]
- Balk D. More than a name: Why is global urban population mapping a GRUMPy proposition? In: Ali G, Hasson S, Khan AM, editors. Global Mapping of Human Settlement: Experiences, Data Sets, and Prospects. Taylor and Francis; Boca Raton, FL: 2009. pp. 145–161. [Google Scholar]
- Balk D, Montgomery MR, McGranahan G, Kim D, Mara V, Todd M, Buettner T, Dorelian A. Mapping urban settlements and the risks of climate change in Africa, Asia and South America. In: Guzman JA, Martine G, McGranahan G, Schensul D, Tacoli C, editors. Population Dynamics and Climate Change. UNFPA; New York: 2009. pp. 80–103. [Google Scholar]
- Balk D, Pozzi F, Yetman G, Deichmann U, Nelson A. The distribution of people and the dimension of place: Methodologies to improve global estimation of urban extents. International Society for Photogrammetry and Remote Sensing Proceedings of the Urban Remote Sensing Conference; Tempe AZ. 2005. [Google Scholar]
- Bocquier P, Madise NJ, Zulu EM. Is there an urban advantage in child survival in sub-Saharan Africa? Evidence from 18 countries in the 1990s. Demography. 2011;48(2):531–558. doi: 10.1007/s13524-011-0019-2. [DOI] [PubMed] [Google Scholar]
- Bocquier P, Beguy D, Zulu EM, Muindi K, Konseiga A, Ye Y. Do migrant children face greater health hazards in slum settlements? Evidence from Nairobi, Kenya. Journal of Urban Health-Bulletin of the New York Academy of Medicine. 2011;88:266–281. doi: 10.1007/s11524-010-9497-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brinkhoff T. City Population. 2014 http://citypopulation.de. [accessed 8 May 2014]
- Brockerhoff M, Brennan E. The poverty of cities in developing regions. Population and Development Review. 1998;24(1):75–114. [Google Scholar]
- Brockerhoff M, Yang X. The impact of migration on fertility in sub-Saharan Africa. Social Biology. 1994;41(1–2):19–43. [PubMed] [Google Scholar]
- Burgert CR, Colston J, Roy T, Zachary B. DHS Spatial Analysis Reports No. 7. Calverton, Maryland, USA: ICF International; 2013. Geographic displacement procedure and georeferenced data release policy for the Demographic and Health Surveys. [Google Scholar]
- Cleves M, Gould W, Gutierrez RG, Marchenko Y. An Introduction to Survival Analysis Using Stata. Third. Stata Press; College Station, Texas: 2010. [Google Scholar]
- Cleland J, Bernstein S, Ezeh A, Faundes A, Glasier A, Innis J. Family planning: the unfinished agenda. The Lancet. 2006;368(9549):1810–1827. doi: 10.1016/S0140-6736(06)69480-4. [DOI] [PubMed] [Google Scholar]
- Cleland J, Wilson C. Demand theories of the fertility transition – an iconoclastic view. Population Studies. 1987;41(1):5–30. [Google Scholar]
- Cohen B. Fertility levels, differentials, and trends. In: Foote KA, Hill KH, Martin LG, editors. Demographic Change in Sub-Saharan Africa. National Academy Press; Washington, DC: 1993. pp. 8–67. [Google Scholar]
- Doll CNH, Pachauri S. Estimating rural populations without access to electricity in developing countries through night-time light satellite imagery. Energy Policy. 2010;38(10):5661–5670. [Google Scholar]
- Dorélien A, Balk C, Todd M. What is urban? Comparing a satellite view with the Demographic and Health Surveys. Population and Development Review. 2013;39(3):413–439. [Google Scholar]
- Easterlin RA. Economic framework for fertility analysis. Studies in Family Planning. 1975;6(3):54–63. [PubMed] [Google Scholar]
- Elvidge CD, Safran J, Nelson IL, Tuttle BT, Hobson VR, Baugh KE, Dietz JB, Erwin EH. Area and position accuracy of DMSP nighttime lights data. In: Lunetta RS, Lyon JG, editors. Remote Sensing and GIS Accuracy Assessment. Taylor and Francis; Boca Raton, Florida: 2004. pp. 355–370. [Google Scholar]
- Fink G, Gunther I, Hill K. Slum residence and child health in developing countries. Demography. 2014;51(4):1175–1197. doi: 10.1007/s13524-014-0302-0. [DOI] [PubMed] [Google Scholar]
- Global Rural-Urban Mapping Project (GRUMP) 2014 http://sedac.ciesin.columbia.edu/data/collection/grump-v1 [accessed May 5, 2014]
- Gould WT. African mortality and the new ‘urban penalty’. Health and Place. 1998;4(2):171–181. doi: 10.1016/s1353-8292(98)00009-4. [DOI] [PubMed] [Google Scholar]
- Gunther I, Harttgen K. Deadly cities? Spatial inequalities in mortality in sub-Saharan Africa. Population and Development Review. 2012;38(3):469–486. [Google Scholar]
- Henderson JV, Storeygard A, Weil DN. Measuring economic growth from outer space. American Economic Review. 2012;102(2):994–1028. doi: 10.1257/aer.102.2.994. [DOI] [PMC free article] [PubMed] [Google Scholar]
- ICF International. Incorporatng Geographic Information into Demographic and Health Surveys: A field guide to GPS data collection. ICF International; Calverton, Maryland: [Google Scholar]
- Jones-Smith J, Popkin BM. Understanding community context and adult health changes in China: Development of an urbanicity scale. Social Science and Medicine. 2010;71(8):1436–1446. doi: 10.1016/j.socscimed.2010.07.027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kirk D, Pillet B. Fertility levels, trends, and differentials in sub-Saharan Africa in the 1980s and 1990s. Studies in Family Planning. 1998;29(1):1–22. [PubMed] [Google Scholar]
- Macro International. DHS-III Basic Documentation No. 6. Calverton, MD: 1996. Sampling Manual. [Google Scholar]
- McGranahan G, Balk D, Anderson B. The rising risks of climate change: Urban population distribution and characteristics in low elevation coastal zones. Environment and Urbanization. 2007;19(1):17–37. [Google Scholar]
- Montgomery MR. Urban poverty and health in developing countries. Population Bulletin. 2009;64(2) [Google Scholar]
- Montgomery MR, Ezeh AC. The health of urban populations in developing countries: An overview. In: Galea S, Vlahov C, editors. Handbook of Urban Health: Population, Methods and Practice. Springer Science; New York: 2005. pp. 201–222. [Google Scholar]
- Mosley WH, Chen LC. An analytical framework for the study of child survival in developing countries. Population and Development Review. 1984;10(suppl):25–45. [PMC free article] [PubMed] [Google Scholar]
- National Research Council. Cities Transformed: Demographic Change and Its Implications in the Developing World. The National Academies Press; Washington, DC: 2003. [Google Scholar]
- Olack B, Burke H, Cosmas L, Bamrah S, Dooling K, Feikin DR, Talley LS, Breiman RF. Nutritional status of under-five children living in an informal urban settlement in Nairobi, Kenya. Journal of Health, Population and Nutrition. 2011;29(4):357–363. doi: 10.3329/jhpn.v29i4.8451. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rutstein S, Rojas G. Guide to DHS Statistics. Calverton, Maryland: 2006. [Google Scholar]
- Schoumaker B. A Stata module for computing fertility rates and TFRs from birth histories: tfr2. Demographic Research. 2013;28:1093–1144. [Google Scholar]
- Shapiro D, Tambashe BO. Fertility transition in urban and rural areas of sub-Saharan Africa: Preliminary evidence of a three-stage process. Journal of Africa Policy Studies. 2002;8:103–127. [Google Scholar]
- United Nations, Department of Economic and Social Affairs, Population Division. World Population Prospects: The 2012 Revision. 2013 http://esa.un.org/unpd/wpp/index.htm.
- United Nations, Department of Economic and Social Affairs, Population Division. World Urbanization Prospects: The 2011 Revision. 2012 http://esa.un.org/unup/
- United Nations Human Settlements Program [UN-Habitat] The State of African Cities 2010: Governance, inequality and urban land markets. Nairobi: UN-Habitat; 2010. [Google Scholar]
- United Nations Human Settlements Program [UN-Habitat] Slums of the world: the face of urban poverty in the new millennium? Monitoring the millennium development goal, Target 11 – worldwide slum dweller estimation. Nairobi: United Nations Human Settlements Program; 2003. [Google Scholar]
- Van de Poel E, O’Donnell O, Van Doorslaer E. What explains the rural-urban gap in infant mortality: household or community characteristics? Demography. 2009;46(4):827–850. doi: 10.1353/dem.0.0074. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wang L. Determinants of child mortality in LDCs: Empirical findings from demographic and health surveys. Health Policy. 2002;65(3):277–299. doi: 10.1016/s0168-8510(03)00039-3. [DOI] [PubMed] [Google Scholar]
- White MJ, Muhidin S, Andrzejewski C, Tagoe E, Knight R, Reed H. Urbanization and fertility: an event-history analysis of coastal Ghana. Demography. 2008;45(4):803–816. doi: 10.1353/dem.0.0035. [DOI] [PMC free article] [PubMed] [Google Scholar]
- WHO/UNICEF Joint Monitoring Programme (JMP) for Water Supply and Sanitation. Progress on sanitation and drinking water: 2010 update. World Health Organization Press; Geneva: 2010. [Google Scholar]