

Sir,
With great interest, we have read article published in your journal in January–March 2017 issue. Urine Albumin Excretion (UAE) as a Marker of Acute Glycemic Changes in Isolated Postprandial Hyperglycemia.[1] The article definitely enlightens about measuring UAE which is relatively easy, less expensive, widely available and done on spot urine samples. In this context, we would like to suggest that using urinary albumin to creatinine ratio (UACR) in spot sample should be performed for measuring albumin excretion in urine.
Urinary excretion of albumin indicates kidney damage and is recognized as a risk factor for the progression of kidney disease and cardiovascular disease. The role of urinary albumin measurements has focused attention on the clinical need for accurate and clearly reported results. Historically, albuminuria has been defined in terms of urinary excretion of albumin per unit time, typically 24 h. The difficulty of collecting 24-h urine samples has led to surrogate measurements of albumin excretion rate. A commonly used surrogate is the ratio of urinary concentrations of albumin and creatinine ratio (ACR).[2]
According to the “The National Kidney Foundation–Kidney Disease Outcomes Quality Initiative guideline for evaluation, classification, and stratification of chronic kidney disease (CKD)” recommends urinary ACR in spot urine samples as the preferred measure rather than urine protein or albumin. The rationale for this recommendation is that ACR is a more sensitive and specific measure of kidney damage.[3]
CKD is diagnosed by the presence of elevated urinary albumin excretion (albuminuria), low estimated glomerular filtration rate (eGFR), or other manifestations of kidney damage. Screening for albuminuria can be most easily performed by UACR in a random spot urine collection. Timed or 24-h collections are more burdensome and add little to prediction or accuracy. The measurement of a spot urine sample for albumin alone (whether by immunoassay or using a sensitive dipstick test specific for albuminuria) without simultaneously measuring urine creatinine (Cr) is less expensive but susceptible to false-negative and false-positive determinations as a result of variation in urine concentration due to hydration. Normal UACR is generally defined as <30 mg/g Cr, and increased urinary albumin excretion is defined as ≥30 mg/g Cr. However, UACR is a continuous measurement, and differences within the normal and abnormal ranges are associated with renal and cardiovascular outcomes. Furthermore, because of biological variability in urinary albumin excretion, two of three specimens of UACR collected within a 3–6-month period should be abnormal before considering a patient to have albuminuria. Exercise within 24 h, infection, fever, congestive heart failure, marked hyperglycemia, menstruation, and marked hypertension may elevate UACR independently of kidney damage. eGFR should be calculated from serum Cr using a validated formula. The CKD Epidemiology Collaboration equation is generally preferred. [Figure 1] Urinary albumin excretion and eGFR each vary within people over time, and abnormal results should be confirmed to stage CKD.[4]
Figure 1.
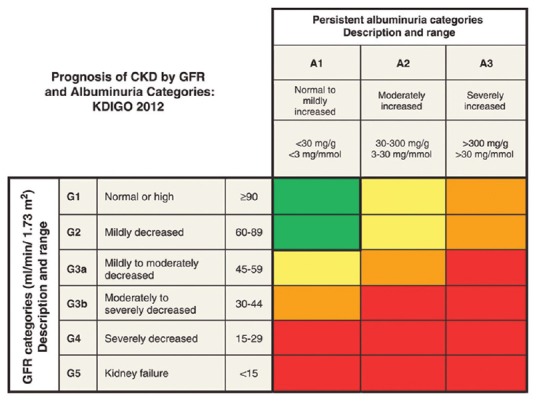
Kidney disease: Improving global outcomes (KDIGO) 2012 Guidelines
Combining eGFR and UACR level was more accurate in predicting the risk of CVD and all-cause mortality. Serum creatinine (eGFR) and urinary ACR should be regularly monitored in diabetic patients. The early intervention to halt or even reverse the progression reduces the risk of CVD and all-cause mortality.[5]
As evidences and guidelines suggest role of eGFR and UACR as renal markers. Clinicians and laboratory Physicians should use these markers appropriately for the benefit of patients. The National Kidney Foundation recommends using the CKD-EPI Creatinine Equation (2009) to estimate GFR. Albumin to creatinine ratio in spot urine sample is used as surrogate marker to estimate albuminuria.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Shilpasree AS, Patil VS, Patil VP, Ingleshwar DG. Urine albumin excretion as a marker of acute glycemic changes in isolated postprandial hyperglycemia. J Lab Physicians. 2017;9:36–41. doi: 10.4103/0974-2727.187925. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Miller WG, Bruns DE, Hortin GL, Sandberg S, Aakre KM, McQueen MJ, et al. Current issues in measurement and reporting of urinary albumin excretion. Clin Chem. 2009;55:24–38. doi: 10.1373/clinchem.2008.106567. [DOI] [PubMed] [Google Scholar]
- 3.Inker LA, Astor BC, Fox CH, Isakova T, Lash JP, Peralta CA, et al. KDOQI US commentary on the 2012 KDIGO clinical practice guideline for the evaluation and management of CKD. Am J Kidney Dis. 2014;63:713–35. doi: 10.1053/j.ajkd.2014.01.416. [DOI] [PubMed] [Google Scholar]
- 4.American Diabetes Association. 10. Microvascular complications and foot care. Diabetes Care. 2017;40(Suppl 1):S88–98. doi: 10.2337/dc17-S013. [DOI] [PubMed] [Google Scholar]
- 5.Fung CS, Wan EY, Chan AK, Lam CL. Association of estimated glomerular filtration rate and urine albumin-to-creatinine ratio with incidence of cardiovascular diseases and mortality in chinese patients with type 2 diabetes mellitus – A population-based retrospective cohort study. BMC Nephrol. 2017;18:47. doi: 10.1186/s12882-017-0468-y. [DOI] [PMC free article] [PubMed] [Google Scholar]