
Fig. 12.
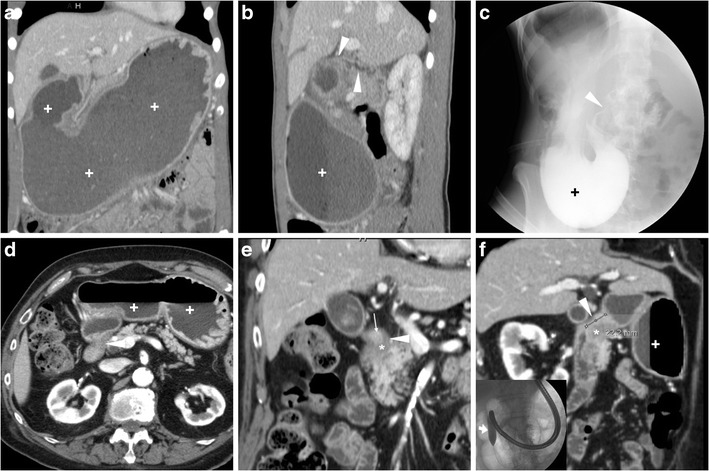
A young 21-year-old female with history of HP infection experienced gastric dilatation, relieved with nasogastric intubation. Despite inability to drink, contrast-enhanced CT (a, b) showed markedly dilated fluid-filled stomach (+), contracted duodenal bulb with 3-cm long stricture (arrowheads in b) without mural thickening, abnormal solid tissue and extrinsic masses. Upper digestive double-contrast fluoroscopy (c) showed dilated stomach with stagnant barium (+) and poorly distensible gastric outlet (arrowhead). Endoscopy confirmed deformed, impassable stricture and two small-sized pyloric ulcers with bioptic finding of severe acute and chronic inflammation. A 88-year-old diabetic male suffered from vomiting, epigastric pain and dark stools. Contrast-enhanced CT (d…f) confirmed radiographic finding of gastric dilatation unrelieved by nasogastric tube, with intraluminal stagnant fluid (+) and depicted a 2-cm pyloric-duodenal stricture (arrowheads in e, f) with subtle submucosal hypoattenuation (*) and mucosal hyperenhancement (thin arrow in e) but no signs of mass-forming or infiltrative disease. Biopsies confirmed post-inflammatory stricture, which was treated by endoscopic dilatation