
Fig. 4.
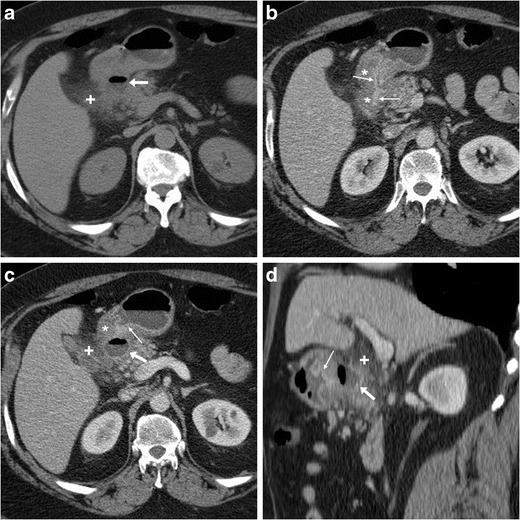
Three months later, the same patient in Fig. 1 experienced severe, recurrent abdominal pain with laboratory evidence of systemic inflammation (14.000/mmc leukocytes, 34 mg/L C-reactive protein). On further questioning, he admitted discontinuation of antacids and H2-blocker medications, and nonsteroidal anti-inflammatory drugs (NSAIDs) intake. Repeated CT revealed increased hypoattenuating mural thickening (*) with mucosal enhancement (thin arrows) of the pylorus and proximal duodenum which spared the anterior aspect, worsened periduodenal inflammatory changes (+), and development of a 2-cm roundish posterior deep ulcer (arrows). Upper digestive endoscopy confirmed a non-malignant retropyloric peptic ulcer. The patient ultimately did well on proton-pump inhibitors (PPI) and anti-Helicobacter pylori triple therapy [Adapted from Open Access ref. no [10]]