
Figure 4.
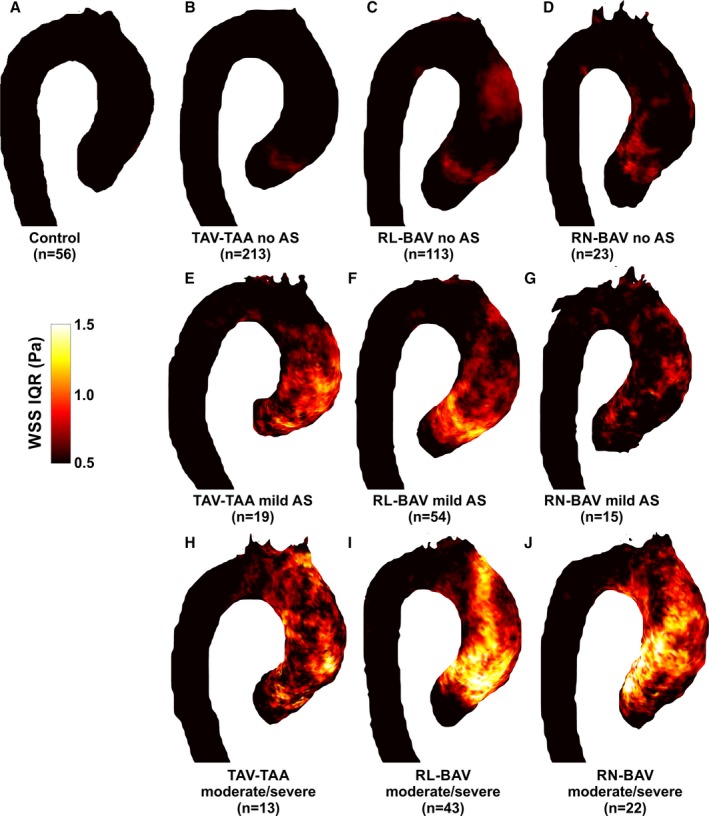
Atlases of WSS interquartile range (IQR) for (A) controls, (B) TAV‐TAA without AS, (C) RL‐BAV without AS, (D) RN‐BAV without AS, (E through G) the corresponding patients with mild AS, and (H through J) the corresponding patients with moderate/severe AS. IQR is expressed as the range between the 75% and 25% quartile of WSS magnitude for all subjects in a given cohort. This represents the regional variability of WSS experienced across the subjects in each group. Controls and patients with no AS (top row) had relatively low WSS variability in the thoracic aorta with mildly elevated WSS IQR in the ascending aorta of BAV patients. In contrast, WSS variability was markedly elevated in the ascending aorta of most AS patient groups (RL‐BAV, RN‐BAV, TAV, and dilated aorta). Color coding=intersubject IQR of WSS magnitude. AS indicates aortic stenosis; BAV, bicuspid aortic valve; RL‐BAV, right and left coronary leaflet fusion BAV; RN‐BAV, right and noncoronary leaflet fusion BAV; TAV‐TAA, tricuspid aortic valve with aortic dilation; WSS, wall shear stress.