

Abstract
Objective
To investigate the prevalence of an excessive prepuce in patients with premature ejaculation (PE) and to evaluate the effectiveness of distal circumcision in reducing the penile hypersensitivity, which is thought to be a cause of PE.
Patients and methods
Men were considered to have an excessive prepuce if the foreskin exceeded the external urethral meatus by ≥1 cm in the flaccid state. The diagnosis of PE was based on the Premature Ejaculation Diagnostic Tool (PEDT) questionnaire score and on the intravaginal ejaculatory latency time (IELT). These features were evaluated at baseline and at 6 months after circumcision.
Results
Lifelong PE was diagnosed in 352 patients of whom 208 (59.1%) had an excessive prepuce. We offered those with an excessive prepuce a circumcision, as a potential definitive treatment for their PE, and 27 (13%) men accepted. At 6 months after circumcision, there was an increase in the mean (SD) IELT from 40.4 (16.5) to 254 (66.8) s (P < 0.001) and the mean (SD) PEDT score decreased from 17 (2) to 6.6 (1.9) (P < 0.001). Overall, 26 of the 27 (96%) patients that had a circumcision reported an IELT increase.
Conclusions
An excessive prepuce is very common in patients affected by PE. Although accepted by only 13% of our patients, distal circumcision was shown to be a very effective surgical treatment for definitive treatment of PE. We therefore recommend assessing patients complaining of lifelong PE for an excessive prepuce and if they have an excessive prepuce to suggest that they undergo distal circumcision.
Abbreviations: IELT, intravaginal ejaculatory latency time; PE, premature ejaculation; PEDT, Premature Ejaculation Diagnostic Tool; SSRI, selective serotonin reuptake inhibitor
Keywords: Circumcision, Excessive prepuce, Penile hypersensitivity, Premature ejaculation, Risk factor
Introduction
Premature ejaculation (PE) is a very common male sexual dysfunction, with a worldwide prevalence of ∼30% [1]. Penile hypersensitivity has been established as a cause of PE [2], [3]. The area of the preputium is considered the most sensitive part of the human penis [4], hence men with an excessive prepuce could be at risk of PE due to higher penile sensitivity. To reduce excessive sensitivity in men with PE, the surgical removal of the prepuce by circumcision could potentially be a definitive treatment for men presenting with an excessive prepuce and complaining of PE [5]. In fact, several published studies have already shown a beneficial effect of circumcision in lengthening the time of sexual intercourse and in reducing symptoms caused by PE [6]. The aims of the present study were: (i) to investigate the prevalence of excessive prepuce in patients with lifelong PE; and (ii) to evaluate the effectiveness of a special type of distal circumcision in ameliorating PE symptoms and on lengthening the intravaginal ejaculatory latency time (IELT) in patients with PE who were diagnosed with an excessive prepuce.
Patients and methods
All patients attending our centre seeking treatment for lifelong PE underwent a meticulous medical and sexual history appraisal and a physical examination. The diagnosis of PE was based on the Premature Ejaculation Diagnostic Tool (PEDT), a self-administered five-item questionnaire validated by Symonds et al. [7], translated and adapted by the author in Italian (Appendix 1). This clinical tool explores all the domains required for a diagnosis of PE, i.e. a lack of ejaculatory control, decreased satisfaction with sexual intercourse, intrapersonal distress, and negative impact on quality of life. The score range for the PEDT is from zero (normal men) to 20 (very severe PE). Men were considered to be affected by PE if the total score was >10. The physical examination was performed for each individual with the aid of a ruler, in a warm room and with the penis in the flaccid state: if the foreskin exceeded the external urethral meatus by ≥1 cm it was considered as an ‘excessive prepuce’ (Fig. 1). We proposed to all patients affected by lifelong PE and presenting with an excessive prepuce that they undergo a distal circumcision as a definitive treatment for their condition. Furthermore, to evaluate the prevalence of excessive prepuce in the normal population, we recorded the number of patients presenting with an excessive prepuce coming to our centre for other urological problems and in whom a diagnosis of PE was excluded (i.e. a PEDT score of ≤10).
Fig. A1.

English version of the Premature Ejaculation Diagnostic Tool (PEDT) questionnaire.
Fig. 1.

Left, typical presentation of an excessive prepuce. Right, aspect of a circumcised penis: a residual portion of foreskin was left to cover the corona glandis when the penis was in a flaccid state.
All patients were evaluated by the same physician (L.G.) and signed an informed-consent form before inclusion. The present study received approval by the ethics committee of our centre.
Exclusion criteria comprised: (i) genital infection; (ii) depression and neurological disorders; (iii) erectile dysfunction (ED), defined as a score from the five-item version of the International Index of Erectile Function (IIEF-5) < 21; (iv) current history of alcohol or drug abuse; (v) use of tricyclic antidepressants, monoamine oxidase inhibitors or selective serotonin re-uptake inhibitors (SSRIs); and (vi) an unstable relationship [8].
Couples that were considered eligible for inclusion underwent a baseline evaluation period of 1 month during which they were asked to have sexual intercourse at least three times, separated by an interval of 24 h, and to record the IELT in a diary card that was provided. To measure IELT, each patient was given a stopwatch and instructed that he, or his partner, should time his IELT for each sexual encounter, by starting timing at vaginal penetration and to stop timing at the start of ejaculation. The baseline IELT for each patient was calculated as the arithmetic mean IELT of all attempts during the first month. After this baseline period, necessary for patient evaluation, distal circumcision surgery was scheduled.
The distal circumcision was performed under local anaesthesia: 20 mL mepivicaine solution injected at the base of the penile shaft. The portion of prepuce to be removed was previously demarcated using a dermographic pen, leaving residual foreskin sufficient to cover only the corona glandis after the surgery (Fig. 1). The distal incision was made very close to the corona glandis (Fig. 2). The ventral incisions were made in a ‘V’ figure in order to perfectly reconstruct the frenulum (Fig. 2, Fig. 3). The prepuce was incised until the deep dartos layer. Blood vessels were carefully coagulated under direct vision. To reduce the excessive sensitivity at the ventral side of the penis a frenulectomy was also performed, using a technique that was already published by our centre [9]. Then the excessive prepuce was removed and a double layer suture with separated sutures was performed: the dartos layer was sutured with 4/0 polyglactin 910 (Vicryl®, Ethicon Endo-Surgery, Cincinnati, OH, USA) and the skin by using 4/0 polyglactin 910 (Vicryl Rapide®, Ethicon Endo-Surgery) (Fig. 2, Fig. 3). A compressive dressing was applied for 48 h. We prescribed 6 days of oral quinolones after surgery.
Fig. 2.

Sequence of images illustrating our surgical technique. The frenulum and the penis raphe were demarcated. The proximal incision was made at the frenulum in figure of ‘V’. The distal incision was performed very close to the corona glandis.
Fig. 3.

Ventral aspect of the circumcised penis: the frenulum area was perfectly reconstructed using a V-shaped proximal incision.
At 6 months after distal circumcision the patients were re-assessed. At this visit every patient again completed the PEDT questionnaire and presented the diary card in which was recorded the IELT for each sexual intercourse during the previous month. For each patient enrolled in our study, we calculated the arithmetic mean values of all PEDT scores and of all IELT measurements.
The main outcome measures were the change in mean IELT and in mean PEDT questionnaire score before and after treatment. For this purpose, we used a t-test for statistical analysis using the Microsoft Excel statistic package.
Results
We diagnosed lifelong PE in 352 patients attending our centre and among them, 208 (59.1%) had an excessive prepuce at physical examination. Overall, during this same period, a diagnosis of an excessive prepuce was confirmed in 601 patients. Among these 601, 208 (34.6%) were affected by PE, while the other 393 (65.4%) came to our centre for other problems. In 80 of the 208 (38.4%) patients diagnosed with PE and presenting an excessive prepuce, a short frenulum was detected as well.
We offered a distal circumcision to all the 208 patients who presented with an excessive prepuce and who were affected by PE as a potential definitive treatment for their problem: 27 (13%) among them accepted. In 20 of these 27 patients (74%) a short frenulum was also detected. At 6 months after circumcision there was an increase in the mean (SD) IELT from 40.4 (16.5) s at baseline to 254 (66.8) s (P < 0.001), while the mean (SD) PEDT score decreased from 17 (2) to 6.6 (1.9) (P < 0.001). In the 20 patients affected by both excessive prepuce and a short frenulum, the mean (SD) IELT increased from 32.1 (8) to 277.4 (61.7) s (P < 0.001) and the mean (SD) PEDT decreased from 17.6 (1.8) to 6.1 (1.5) (P < 0.001). In the seven patients presenting only with an excessive prepuce, the mean (SD) IELT increased from 64.1 (9.6) to 187.1 (16) s (P < 0.001) and the mean (SD) PEDT score decreased from 15.1 (1) to 8.1 (2.2) (P < 0.001). Overall, the mean IELT increased after distal circumcision by 764.2% (from 32.1 to 277.4 s) in patients affected by both an excessive prepuce and a short frenulum and by 191.9% (from 64.1 to 187.1 s) in individuals presenting only with an excessive prepuce. Overall, the mean PEDT score decreased after distal circumcision by 65.9% (from 17.6 to 6.1) in patients with both an excessive prepuce and a short frenulum and by 46.3% (from 15.1 to 8.1) in men presenting with only an excessive prepuce. In all, 26 of the 27 patients (96%) reported an increase in their IELT, while there was no change in only one man. All patients who underwent distal circumcision with our surgical technique reported an aesthetic improvement with a better perception of their body image and described a significant amelioration in their personal care. Results are shown in Fig. 4, Fig. 5.
Fig. 4.
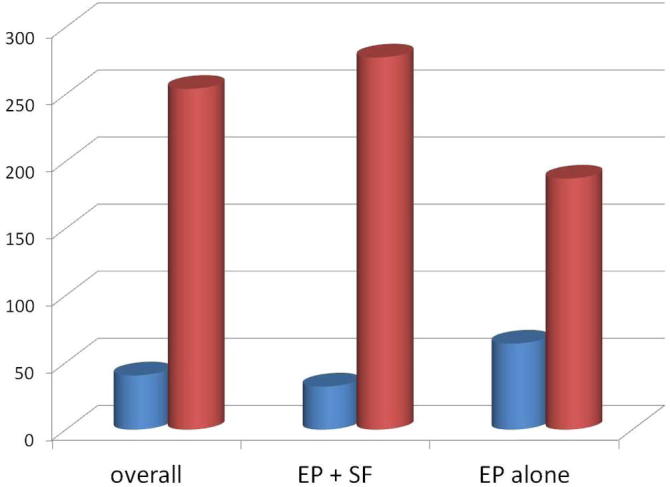
The mean IELT before and after circumcision (s). EP, excessive prepuce; SF, short frenulum.
Fig. 5.
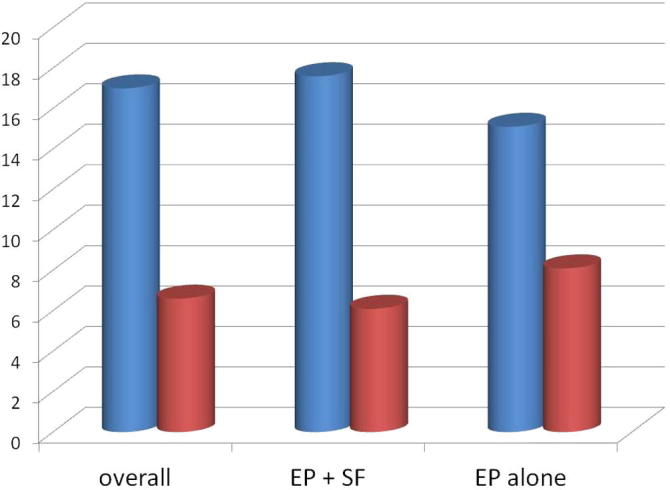
The mean PEDT score before and after circumcision. EP, excessive prepuce; SF, short frenulum.
Discussion
PE therapy is usually based on two classes of drugs: topical anaesthetics and SSRIs [10]. Unfortunately, both these medications are not definitive treatments for PE and their use has been associated with adverse reactions [11], [12], [13].
Penile hypersensitivity is one of the ascertained causes of PE [2], [3]. The prepuce is an anatomical structure of the male external genitalia of all human and non-human primates [14]. The normal length of the prepuce is 6.4 cm (range 4.8–9.2 cm), occupying 93% of the penile shaft [15]. The prepuce is a simple fold of skin composed of outer keratinised skin and an inner mucosal layer, which is very rich in nerves [4]. The prepuce is highly sensitive due to the abundance of nerve fibres, which underlies its function as an erogenous tissue. The Canadian pathologist John Taylor [4] was the first to study the area of the prepuce usually removed by circumcision. He defined this area as the ‘ridged band’ and found that this anatomical structure was the most sensitive part of the human penis, containing more Meissner’s corpuscles than smooth mucosa and therefore exhibiting features of specialised sensory mucosa.
Circumcision is a surgical procedure in which the prepuce is removed. It has been performed since the times of ancient Egypt for various reasons, which can broadly be categorised into: medical, religious, cultural, and social. Circumcision in all newborns is a religious requirement for the Islamic and Jewish communities, and for many African populations. In Western countries the most prevalent indication for circumcision is as therapy for phimosis, but it also is performed for functional reasons and in some cases for aesthetic reasons [16]. Recently, the American Academy of Pediatrics stated that ‘the health benefits of newborn male circumcision outweigh the risks’ [17]. In fact it was shown that circumcision can aid in the prevention of UTIs, acquisition of HIV, transmission of some sexually transmitted infections, and penile cancer [18].
The surgical ablation of the prepuce removes many of the corpuscular receptors from the penis [4], [19]. Sorrells et al. [5] used a Semmes-Weinstein monofilament touch test to compare the fine-touch pressure thresholds of the penis in 159 adult male volunteers with no history of penile pathology. They found that the glans of uncircumcised men had significantly lower mean pressure thresholds than those of the circumcised men, concluding that the circumcised penis is less sensitive than the uncircumcised penis. In that same study the high sensitivity of the frenulum area was also demonstrated, confirming the previous findings of Halata and Munger [20].
Several published studies have shown that in some cases circumcision, thereby reducing the sensitivity of the penis, can provide benefits to sexual health. Senol et al. [21] concluded that circumcision may, by prolonging pudendal evoked potentials latency, contribute to sexual satisfaction. Senkul et al. [6] reported that adult circumcision did not adversely affect sexual function, assessed using the Brief Male Sexual Function Inventory (BMSFI) questionnaire, and that the increase in the IELT could be considered an advantage rather than a complication. In the study by Namavar and Robati [22], the surgical removal of foreskin remnants in adults previously circumcised resulted in a significant improvement in the IELT. The patients evaluated in that study reported improvements in the frequency of intercourse/week, a better appearance of their penis after surgery, and increased partner satisfaction. Cortés-González et al. [23] reported that after circumcision there was a reduction in PE frequency, from 31.8% to 13.6%, in a group of 22 heterosexual male adults who were sexually active with a stable partner. Alp et al. [24] reported statistically significantly increased IELTs and reduced PEDT scores in 30 volunteers after circumcision. Waldinger et al. [25] reported in their study of 500 males, that the mean IELT was 6 min in uncircumcised males vs 6.7 min in circumcised males. A Chinese prospective randomised multicentre study investigated the effects of circumcision on PE evaluating 575 circumcised men and 623 uncircumcised men. The circumcised men reported significantly improved IELT, control over ejaculation, and satisfaction with sexual intercourse, suggesting that circumcision might have positive effects on the IELT, ejaculatory control, sexual satisfaction and PE severity [26].
Therefore, the use of circumcision for the treatment of lifelong PE is based on two main assumptions: firstly, several published studies have shown that circumcision, results in a desensitisation of the glans, thus improving the IELT. Secondly, circumcision is a potential definitive treatment for PE whereas the other on-demand medical therapies are palliative.
To the best of our knowledge the present is the first study investigating the prevalence of excessive prepuce and the effect of circumcision in such cases for the treatment of PE.
In the present study, it was found that an excessive prepuce is very common in patients with lifelong PE: overall the 59.1% of patients complaining of PE had an excessive prepuce. This high prevalence may reflect a scientific explanation in that men with an excessive prepuce have higher penis sensitivity, as the foreskin, as extensively discussed before, is the most sensitive part of the human penis. However, PE is a multi-factorial disease whose aetiology is not yet completely established. An excessive prepuce is obviously not the only cause of PE, as 393 men in which an excessive prepuce was identified did not have PE. In 80 patients among the 208 (38.4%) with PE and presenting with an excessive prepuce, a concomitant short frenulum was also identified, which is another condition that is a risk factor for PE [9]. Overall the prevalence of an excessive prepuce in patients affected by PE in the present study was of the 59.1%, higher than the prevalence of a short frenulum in the same type of patients (43%). Only 27 patients among the 208 who were diagnosed with an excessive prepuce and PE agreed to undergo circumcision and only seven among these 208 (3.3%) presented with an excessive prepuce alone, while the other 20 had both an excessive prepuce and a short frenulum. As already reported in another trial, even these data confirm that Italian patients affected by PE are very reticent to undergo circumcision even if this surgical procedure may provide a definitive treatment for their problem [27]. Instead, the concomitant presence of both these PE risk factors seems to be a more convincing reason for patients to accept circumcision surgery. This finding is consistent with our previous findings: 40 among 45 men (89%) diagnosed with a short frenulum and PE accepted to undergo frenulectomy [9]. At 6 months after circumcision, we found an impressive increase in the mean IELT of 535% (from 40 to 254 s) and a dramatic drop of 61.2% in the mean PEDT score (from 17 to 6.6). In the previous study, we found that frenulectomy in patients affected by PE and presenting with a short frenulum had a mean IELT increase of 149% (from 1.65 to 4.11 min) and reduction in the mean PEDT of 37.6% (from 15.8 to 9.85). In the 20 patients in the present study affected by both an excessive prepuce and a short frenulum, we found an even higher increase in the mean IELT of 764.2% (from 32.1 to 277.4 s) and a more consistent reduction in the PEDT score of 65.9% (from 17.6 to 6.1). Therefore we can conclude that circumcision associated with frenulectomy is more effective than frenulectomy alone for the treatment of lifelong PE, as circumcision removes more sensitive tissue rich in nerve fibres.
At this juncture, we should also recognise that some published studies have found that the reduction of penis sensitivity caused by circumcision can lead to deleterious effects on male sexuality. Adverse self-reported outcomes associated with foreskin removal in adulthood include impaired erection, orgasm difficulties, decreased masturbatory functioning, increase in penile pain, and loss of penile sensitivity [28], [29], [30], [31]. Kim et al. [32] found that circumcised men reported decreased masturbatory pleasure and sexual enjoyment, and concluded that adult circumcision adversely affects sexual function in a substantial number of men due to the loss of nerve endings. Also, 9% of the circumcised men reported severe scarring of their penises. In the same study, there were no significant differences in sexual drive, erection, ejaculation, and IELT between circumcised and uncircumcised men. However, that study presents the limitation of not precisely reporting both the amount and the portion of the removed foreskin. In fact, as described by Eid [33], it is possible to perform a ‘cosmetic circumcision’ by removing the skin at the level of the base of the penis. This type of circumcision would obviously not be effective for the therapy of PE, as it removes a portion of penile skin that is much less sensitive than the distal prepuce. Moreover, as described by Namavar et al. [22], further removal of foreskin in men already circumcised resulted in a significant increase in the IELT. Our surgical technique provides a generous removal of the preputial tissue (including the dartos layer), as we left just a portion of the foreskin to cover the corona and we executed the distal incision very close to the glans in order to remove the Taylor’s ridged band, the most sensitive part of the penis (Fig. 1, Fig. 2).
Furthermore, we proposed and performed a distal circumcision in a very select cohort of patients for whom there was strong scientific basis for success: patients affected by life-long PE, presenting with an excessive prepuce, and who were willing to undergo a definitive treatment for their problem.
We admit that the absence of a control group represents a limitation of the present study. We encourage further two-arm prospective studies in which two different circumcision techniques removing different parts of the prepuce are compared (proximal and/or central circumcision vs distal circumcision).
Conclusions
We can conclude that adult distal circumcision, resulting in a consistent reduction in penile sensitivity, is a strong weapon in the hands of urological surgeons, which must be used very carefully, as its effects on male sexuality can be devastating and irreversible if performed in the wrong patient. Thus, the caveat must be ‘do the right circumcision in the right patient using the correct surgical technique’. The present study shows that an excessive prepuce is an organic risk factor for PE, as already shown for prostatitis and for a short frenulum [9], [34].
An excessive prepuce is very common in patients with PE. Although accepted by only 13% of our present cohort, distal circumcision was shown to be a very effective surgical treatment for PE. Based on our present findings, we suggest assessing patients complaining of lifelong PE for an excessive prepuce, and if present, to suggest that they undergo a distal circumcision.
Conflicts of interest
None.
Andrology/Sexual Medicine
Footnotes
Peer review under responsibility of Arab Association of Urology.
Appendix A
See Fig. A1.
References
- 1.Carson C., Gunn K. Premature ejaculation: definition and prevalence. Int J Impot Res. 2006;18(Suppl. 1):S5–S13. doi: 10.1038/sj.ijir.3901507. [DOI] [PubMed] [Google Scholar]
- 2.Xin Z.C., Chung W.S., Choi Y.D., Seong D.H., Choi Y.J., Choi H.K. Penile sensitivity in patients with primary premature ejaculation. J Urol. 1996;156:979–981. [PubMed] [Google Scholar]
- 3.Xin Z.C., Choi Y.D., Rha K.H., Choi H.K. Somatosensory evoked potentials in patients with primary premature ejaculation. J Urol. 1997;158:451–455. [PubMed] [Google Scholar]
- 4.Taylor J.R., Lockwood A.P., Taylor A.J. The prepuce: specialized mucosa of the penis and its loss to circumcision. Br J Urol. 1996;77:291–295. doi: 10.1046/j.1464-410x.1996.85023.x. [DOI] [PubMed] [Google Scholar]
- 5.Sorrells M.L., Snyder J.L., Reiss M.D., Eden C., Milos M.F., Wilcox N. Fine-touch pressure thresholds in the adult penis. BJU Int. 2007;99:864–869. doi: 10.1111/j.1464-410X.2006.06685.x. [DOI] [PubMed] [Google Scholar]
- 6.Senkul T., IşerI C., şen B., KarademIr K., Saraçoğlu F., Erden D. Circumcision in adults: effect on sexual function. Urology. 2004;63:155–158. doi: 10.1016/j.urology.2003.08.035. [DOI] [PubMed] [Google Scholar]
- 7.Symonds T., Perelman M.A., Althof S., Giuliano F., Martin M., May K. Development and validation of a premature ejaculation diagnostic tool. Eur Urol. 2007;52:565–573. doi: 10.1016/j.eururo.2007.01.028. [DOI] [PubMed] [Google Scholar]
- 8.Rosen R.C., Cappelleri J.C., Smith M.D., Lipsky J., Pena B.M. Development and evaluation of an abridged, 5-item version of the International Index of Erectile Function (IIEF-5) as a diagnostic tool for erectile dysfunction. Int J Impot Res. 1999;11 doi: 10.1038/sj.ijir.3900472. 319–266. [DOI] [PubMed] [Google Scholar]
- 9.Gallo L., Perdonà S., Gallo A. The role of short frenulum and the effects of frenulectomy on premature ejaculation. J Sex Med. 2010;7:1269–1276. doi: 10.1111/j.1743-6109.2009.01661.x. [DOI] [PubMed] [Google Scholar]
- 10.EAU. Guidelines on Male Sexual Dysfunction: Erectile dysfunction and premature ejaculation. Available at: http://uroweb.org/guideline/male-sexual-dysfunction/. Accessed March 2017. [DOI] [PubMed]
- 11.Morales A., Barada J., Wyllie M.G. A review of the current status of topical treatments for premature ejaculation. BJU Int. 2007;100:493–501. doi: 10.1111/j.1464-410X.2007.07051.x. [DOI] [PubMed] [Google Scholar]
- 12.Rosen R.C., Lane R.M., Menza M. Effects of SSRIs on sexual function: a critical review. J Clin Psychopharmacol. 1999;19:67–85. doi: 10.1097/00004714-199902000-00013. [DOI] [PubMed] [Google Scholar]
- 13.Buvat J., Tesfaye F., Rothman M., Rivas D.A., Giuliano F. Dapoxetine for the treatment of premature ejaculation: results from a randomized, double-blind, placebo-controlled phase 3 trial in 22 countries. Eur Urol. 2009;55:957–967. doi: 10.1016/j.eururo.2009.01.025. [DOI] [PubMed] [Google Scholar]
- 14.Cold C.J., Taylor J.R. The prepuce. BJU Int. 1999;83:34–44. doi: 10.1046/j.1464-410x.1999.0830s1034.x. [DOI] [PubMed] [Google Scholar]
- 15.Hsieh T.F., Chang C.H., Chang S.S. Foreskin development before adolescence in 2149 schoolboys. Int J Urol. 2006;13:968–970. doi: 10.1111/j.1442-2042.2006.01449.x. [DOI] [PubMed] [Google Scholar]
- 16.Morris B.J., Krieger J.N. Does male circumcision affect sexual function, sensitivity, or satisfaction? A systematic review. J Sex Med. 2013;10:2644–2657. doi: 10.1111/jsm.12293. [DOI] [PubMed] [Google Scholar]
- 17.American Academy of Pediatrics Task Force on Circumcision Circumcision policy statement. Pediatrics. 2012;130:585–586. [PubMed] [Google Scholar]
- 18.American Academy of Pediatrics Task Force on Circumcision Male circumcision. Pediatrics. 2012;130:e756–e785. [Google Scholar]
- 19.Fink K.S., Carson C.C., DeVellis R.F. Adult circumcision outcomes study: Effect on erectile function, penile sensitivity, sexual activity and satisfaction. J Urol. 2002;167:2113–2116. [PubMed] [Google Scholar]
- 20.Halata Z., Munger B.L. The neuroanatomical basis for the protopathic sensibility of the human glans penis. Brain Res. 1986;371:205–230. doi: 10.1016/0006-8993(86)90357-4. [DOI] [PubMed] [Google Scholar]
- 21.Senol M.G., Sen B., Karademir K., Sen H., Saraçoğlu M. The effect of male circumcision on pudendal evoked potentials and sexual satisfaction. Acta Neurol Belg. 2008;108:90–93. [PubMed] [Google Scholar]
- 22.Namavar M.R., Robati B. Removal of foreskin remnants in circumcised adults for treatment of premature ejaculation. Urol Ann. 2011;3:87–92. doi: 10.4103/0974-7796.82175. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Cortés-González J.R., Arratia-Maqueo J.A., Martínez-Montelongo R., Gómez-Guerra L.S. Does circumcision affect male's perception of sexual satisfaction? Arch Esp Urol. 2009;62:733–736. doi: 10.4321/s0004-06142009000900008. [DOI] [PubMed] [Google Scholar]
- 24.Alp B.F., Uguz S., Malkoc E., Ates F., Dursun F., Okcelik S. Does circumcision have a relationship with ejaculation time? Premature ejaculation evaluated using new diagnostic tools. Int J Impot Res. 2014;26:121–123. doi: 10.1038/ijir.2013.47. [DOI] [PubMed] [Google Scholar]
- 25.Waldinger M.D., Quinn P., Dilleen M., Mundayat R., Schweitzer D.H., Boolell M. A multinational population survey of intravaginal ejaculation latency time. J Sex Med. 2005;4:492–497. doi: 10.1111/j.1743-6109.2005.00070.x. [DOI] [PubMed] [Google Scholar]
- 26.Gao J., Xu C., Zhang J., Liang C., Su P., Peng Z. Effects of adult male circumcision on premature ejaculation: results from a prospective study in China. Biomed Res Int. 2015;2015:417846. doi: 10.1155/2015/417846. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Gallo L. Patients affected by premature ejaculation due to glans hypersensitivity refuse circumcision as a potential definite treatment for their problem. Andrologia. 2014;46:349–355. doi: 10.1111/and.12083. [DOI] [PubMed] [Google Scholar]
- 28.Bossio J.A., Pukall C.F., Steele S. A review of the current state of the male circumcision literature. J Sex Med. 2014;11:2847–2864. doi: 10.1111/jsm.12703. [DOI] [PubMed] [Google Scholar]
- 29.Bronselaer G.A., Schober J.M., Meyer-Bahlburg H.F., T'Sjoen G., Vlietinck R., Hoebeke P.B. Male circumcision decreases penile sensitivity as measured in a large cohort. BJU Int. 2013;111:820–827. doi: 10.1111/j.1464-410X.2012.11761.x. [DOI] [PubMed] [Google Scholar]
- 30.Frisch M., Lindholm M., Grønbeck M. Male circumcision and sexual function in men and women: a survey-basedcross-sectional study in Denmark. Int J Epidemiol. 2011;40:1367–1381. doi: 10.1093/ije/dyr104. [DOI] [PubMed] [Google Scholar]
- 31.Dias J., Freitas R., Amorim R., Espiridião P., Xambre L., Ferraz L. Adult circumcision and male sexual health: a retrospective analysis. Andrologia. 2014;46:459–464. doi: 10.1111/and.12101. [DOI] [PubMed] [Google Scholar]
- 32.Kim D., Pang M.G. The effect of male circumcision on sexuality. BJU Int. 2007;99:619–622. doi: 10.1111/j.1464-410X.2006.06646.x. [DOI] [PubMed] [Google Scholar]
- 33.Eid J.F. The cosmetic circumcision. J Sex Med. 2013;10:2129–2132. doi: 10.1111/jsm.12289. [DOI] [PubMed] [Google Scholar]
- 34.Shamloul R. Chronic prostatitis in premature ejaculation: A cohort study in 153 men. J Sex Med. 2006;3:150–154. doi: 10.1111/j.1743-6109.2005.00107.x. [DOI] [PubMed] [Google Scholar]