

Abstract
Introduction: The purpose of this study was to investigate the effect of low-level laser therapy (LLLT) – 660 nm and 904 nm - before grip strength protocol in healthy subjects.
Methods: The study included 45 healthy volunteers with an average age of 22.7 (±1.4) years, subdivided into the following groups, control group: grip strength training associated with placebo LLLT; 660 nm group: LLLT (660 nm, 20 J/cm2, power of 30 mW, and beam area of 0.06 cm2, continuous, energy 1.2 J, and exposure time 40 seconds per point) before grip strength training and 904 nm group: LLLT (904 nm, 10 J/cm2, peak power of 70 W and 0.13 cm2 beam area, with pulsed beam 9.500 Hz and 30 seconds of exposure time per point and emitted energy 1.2 J) before grip strength training. The LLLT was timed to contact 10 points located in the region of the superficial and deep flexor muscles of the fingers, with a total energy of 12.0 J per session. For the strength training protocol, the volunteer exercised their fingers with the dominant hand on a small table, elbow flexed at 90°, forearm in neutral, using a light extension handle. The Oxford protocol was performed during four weeks. The grip strength was assessed using a dynamometer (Jamar™). The data were evaluated by the analysis of variance (ANOVA) statistical method.
Results: In the comparison of intragroup evaluation, only the 904 nm group showed a difference compared to the baseline assessment after 4 weeks (P < 0.05), in the final intergroup evaluation, a difference was observed in the comparison between the control and 904 nm groups
Conclusion: In conclusion, LLLT (904 nm) applied before resistance training was effective in gaining grip strength when compared to LLLT (660 nm) and isolated strength training after 4 weeks.
Keywords: Laser Therapy, Low-Level, Hand Strengths, Therapy, Photobiomodulation
Introduction
Upper limb anatomy is considered complex due to the large number of structures present in this segment, such as bone, ligaments, muscles, flexor tendons/extensors, intrinsic muscles, peripheral nerves, blood vessels, and tegument.1,2 Among the body segments, hands play a fundamental role due to the varieties of work they do and the extreme precision of their movements. People with grip disorders present impairment in activities of daily living that require the return of power to this body segment.
Bawa et al,3 describe synergism between wrist extensors and flexors. Extensor muscles stabilize wrist in extension position during hand grip and studies that investigate this synergic relation in functional activities are important to understand the physiopathology and to delineate prevention and treatment protocols in musculoskeletal dysfunctions like lateral epicondylitis. A decrease in grip strength may be related to several diseases, such as fracture of the radius, damage to the central and peripheral nervous system, among others.4-8
Studies using therapeutic resources (kinesiotherapy and electrophysical agents) have great importance due to their applicability in clinical practice, aiming to promote early restoration of functionality in the rehabilitation of the hand and upper limb.9,10 Phototherapy has been widely used in research of different tissues, such as tendons, peripheral nerve, skin tissue, bones, and muscle.11-16
In this context, low-level laser therapy (LLLT), and light emitting diode therapy (LEDT) are efficient on bioenergetics muscle activation, and these effects may influence performance during physical activities. Therefore, researchers started to investigate LLLT and LEDT as a way to improve muscle performance as LLLT and LEDT induce photochemical effects on cells by light absorption at photoreceptors;phenomenon described as photobiomodulation. This phenomenon is characterized by the cellular capacity to interact with certain types of light according to its wavelength, energy density, and potency.
Thus, researchers investigated the use of these resources as a method to promote improvement of muscle performance, delay of fatigue, muscle strength, and prevention of muscle injuries. Phototherapy associated with resistance exercise protocols or muscular endurance has shown positive results, better than when performed in different groups, improving performance, endurance, and recovery from fatigue, proven by the various strength tests and the biomarker analyses such as lactate, creatine kinase, and C-reactive protein.16-25
Leal-Junior et al18 made a systematic review about LLLT/LEDT effects on performance among exercise, and at recovery markers after muscle fatigue. The study concludes that results more significant, and consistent, occurred with red or infrared wavelengths applied before exercise. Although studies, mostly evaluate group muscles, as femoral quadriceps and biceps brachialis, these effects on the forearm, wrist, and hand were not previously analyzed.
Based on this context, it is believed that LLLT emission before the strength protocol will improve muscle performance. The present study aims to investigate the effect of LLLT – 660 nm and 904 nm – before grip strength protocol in healthy subjects.
Purpose of the Study
The study was characterized as randomized controlled, with a proposal for evaluation and intervention through the effect of LLLT, coupled with strength training of the fingers’ flexor muscles.
Methods
Subjects
The sample consisted of subjects who fulfilled the inclusion criteria, all of 45 subjects were females. The subjects were divided into the following groups:
Control group: grip strength training associated with placebo LLLT;
660 nm: grip strength training associated with LLLT 660 nm;
904 nm: grip strength training associated with LLLT 904 nm (Figure 1).
Figure 1.

Flow Diagram Showing the Recruitment Process and the Reasons for Exclusion.
Inclusion Criteria
Individuals above 18 years old were selected, female, with no regular physical activity.
Exclusion Criteria
Individuals with complaints of pain in the arm or who had nerve damage associated with multiple complex lesions, bone or joint injuries, the presence of central nervous system injury, rheumatic diseases, leprosy, and diseases affecting the upper limbs. All evaluated subjects did not present any of these criteria.
Recruitment, Collection, Location, and Staff
The proposed intervention and purpose of the study was explained to the volunteers and also presented in the informed consent form. After reading and signing this form, participation in the study was considered voluntary. Following this, a physical and functional evaluation was performed. Evaluations were made at the clinical-school institution, at baseline and after eight sessions of the protocol.
The randomization to groups was based on a sequence of random numbers generated using Excel®.
The team was composed of 4 undergraduates in physiotherapy at each University, as follows: one person for the intervention, two for recruitment, and a blind evaluator.
The evaluation was performed by a hand therapist (a member of the Brazilian Society of Hand Therapy – BSHT) with experience in the evaluation and treatment of upper limb disorders.
The evaluation was based on items related to function and muscle strength. Isometric muscle strength of grip of the fingers was assessed by isometric dynamometry (Jamar®).
Proposal for Intervention
Evaluation
The task performed by the volunteers was to grip with the dominant limb using the dynamometer (Jamar®). The positioning of the individual to assess the handgrip followed the recommendation given by the American Society of Hand Therapists (ASHT) and the Brazilian Society of Hand Therapists (BSHT), based on the studies of Mathiowetz et al.26 The individual was positioned comfortably in a chair without support for the arms, feet flat on the floor, parallel to the body arm, shoulder adducted, elbow at 90o and forearm in neutral position, and the Jamar® dynamometer in second place.27 The evaluation was performed in both groups at baseline and after the end of the experiments (Figure 2).
Figure 2.

Assessment of Grip Strength With Dynamometer (Jamar™).
Emitting Laser Radiation Equipment
Diode laser equipment indium gallium aluminum phosphorus (InGaAlP) was used with a wavelength of 660 nm, fluence of 20 J/cm2, power of 30 mW, and beam area of 0.06 cm2, using the continuous beam of the Ibramed™, issued energy (E) = 1.2 J, and exposure time 40 seconds per point. Also used was a wavelength of 904 nm gallium arsenide (GaAs), fluence 10 J/cm2, peak power of 70 W (average power 0.04 W) and 0.13 cm2 beam area, with pulsed beam (9.500 Hz) and 30 seconds of exposure time per point and emitted energy (E) = 1.2 J. Laser radiation was timed to contact in 10 points located in the region of the superficial and deep flexor muscles of the fingers, using a total energy of 12.0 J per session. The control group had simulated irradiation with the equipment switched off for 30 seconds per point (Figure 3).
Figure 3.
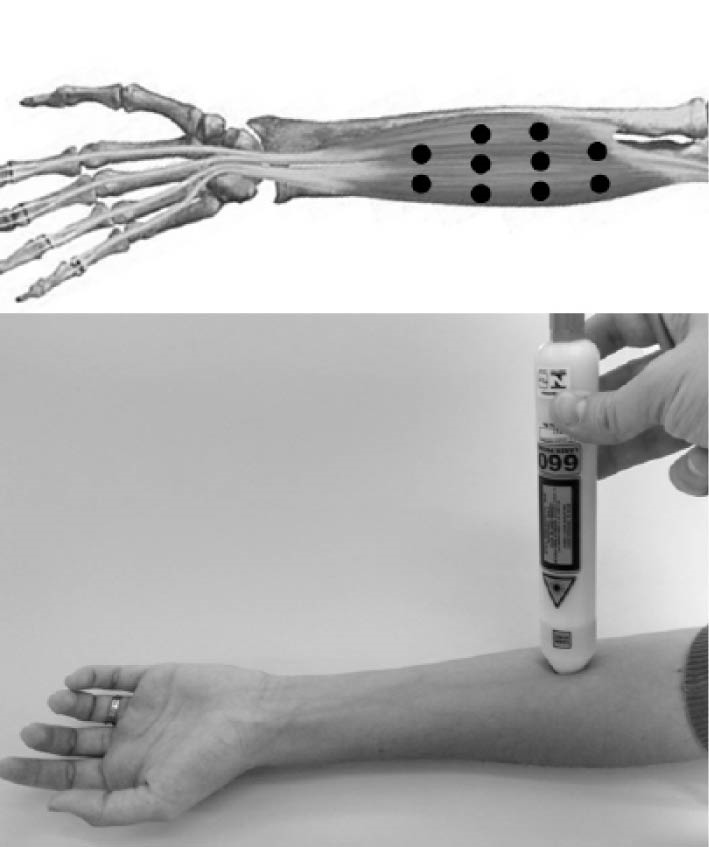
Points of LLLT Irradiation on the Extrinsic Flexors of Forearm.
Individuals submitted to the LLLT protocol, performed 2 weekly sessions with a total of eight pre-training strength applications.
Laser emission measurement was carried out at baseline and after the end of the experiments.
Strengthening Protocol
For the strength training protocol of the dominant limb, a finger exerciser was used, with the volunteer’s arm resting on a table, elbow flexed at 90°, forearm in neutral, with a light extension handle. This calculated the maximum resistance (10 MR) of the flexor fingers. Afterwards, the Oxford protocol was performed starting with 10 repetitions at 100% of 10 RM, followed by 10 repetitions at 75% of 10 RM and, finally, 10 repetitions at 50% 10 RM load.10 Two weekly sessions were conducted over 4 weeks.
Statistical Analysis
The sample calculation was based on the standard deviation of a pilot study using GraphPad StatMate software.
All statistical procedures were performed through Biostate® 5.0 software. Prior to the analysis of each group, the normal distribution of the data was verified by means of descriptive statistical procedures, using the Shapiro-Wilk test.
After collection, the average strength data of the groups were subjected to statistical analysis by the analysis of variance (ANOVA) test with alpha P < 0.05, evidenced by the post-hoc Tukey test.
Results
Of the initial sample of 45 subjects, none reported any pain or discomfort during the data collection. Two volunteers were excluded for not completing the protocol, totaling 43 individuals. The characteristics of the sample are shown in Table 1.
Table 1. Participant Characteristics at Baseline .
| Characteristic | Sham | 660 | 904 |
| Voluntary = n | 15 | 15 | 15 |
| Age (y), mean (SD) | 22.6 (1.3) | 22.7 (1,5) | 22.9 (1,2) |
| Hand dominance | Right=12; Left= 3 |
Right=12; Left= 2 |
Right = 13; Left = 1 |
| Work status: FT/PT/ NW | NW = 15 |
PT = 1; NW= 14 |
NW= 15 |
| VAS | 0 | 0 | 0 |
Abbreviations: SD, standard deviation; FT; full time; PT, part time; NW, not working; VAS, visual analog scale.
The assessment of grip strength was similar at baseline for all groups, with no statistically significant difference between them.
In the intragroup evaluation, grip strength increased significantly only for the 904 nm group which showed a difference in comparison to the baseline assessment after 4 weeks.
In the final intergroup evaluation, a difference was observed in the comparison between the control and 904 nm groups. This can be seen in Figure 4.
Figure 4.
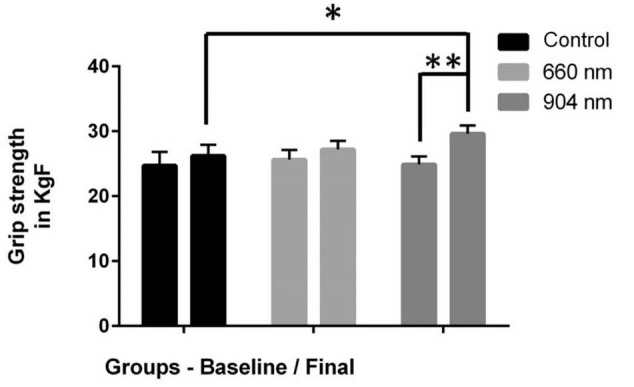
Grip Strength of Different Groups (KgF) Comparing Baseline and Final Assessments. *Intergroup difference, ** Intragroup difference (p<0.05, 95=""% CI).=""
Discussion
The aim of this study was to evaluate LLLT effects on grip strength. The protocol has shown to be efficient in improving the grip strength. This condition was more evident in 904 nm, in which there was a difference between the final and baseline. Thereby, it can be suggested that, for 904 nm group, irradiation was efficient to improve the grip strength. Volunteers well accepted the evaluation protocol and treatment;no complaint was recorded about evaluation time or LLLT application.
Among the body segments, hands play a fundamental role due to the varieties of work they do and the extreme precision of their movements. People with grip disorders present impairment in activities of daily living, requiring the therapist to engage in returning strength to that body segment. In this study, the use of LLLT 904 nm optimized gain strength in healthy subjects when associated with a four week strengthening protocol.
Fernandes et al10 performed an isotonic strengthening program to increase grip strength. They applied the protocols of Oxford and DeLorme in healthy patients to check the grip strength gain and reached the conclusion that both protocols were helpful and, therefore, valid for grip strength recovery. The authors concluded that for effective rehabilitation it is not enough to establish a protocol to gain muscle strength, but a way must be found to assess the gain with a valid instrument, such as a held dynamometer. This study reproduced this methodology for the strengthening protocol and it has been well accepted by all individuals without any complaints of pain or discomfort during its use.
Leal-Junior et al,18 in a systematic review with meta-analysis, considered the phototherapy effects (LLLT and LEDT) on exercise performance and muscle recovery. In this study, 13 articles were reviewed that demonstrated this effect in different body segments (5 rated the biceps, 7 rated muscles of the quadriceps, and 1 rated the masseter). Thus, our study is unprecedented with respect to the evaluation of the muscles involved in handgrip activity and enables the development of new studies relating phototherapy with strength training and its application in various lesions that may lead to decreased strength in this segment, for example, as a result of radius fractures, injuries of the flexor tendons of fingers, and hand complex lesions.
Nampo et al,28 investigated if LLLT improves exercise capacity and muscle performance. The review used sixteen studies that analyzed pre exercise LLLT or LEDT irradiation effects with different parameters. It analyzed contraction repetition number, time to exhaustion, blood lactate concentration, lactate dehydrogenase activity, muscle peak torque, muscle power and muscle strength, corroborating our findings regarding the force improvement.
Larger wavelengths allow irradiation in deep strata due to the higher penetration power, justifying the best result recorded in strength gain by the group 904 nm with respect to 660 nm. The effectiveness of the light LLLT near 660 nm and 904 nm, has been implicated in the resolution of skin injury and traumatic lesions, such as lesions of the peripheral nervous system,29-31 but showed no favorable results in the present study. However, other authors have demonstrated positive effects of LLLT and LEDT in this wavelength range on muscle performance.32-33
Ferraresi et al,34 investigated the use of LLLT associated with strength training using leg-press exercises twice a week for 12 consecutive weeks. After each session, the LLLT group was subjected to the application of LLLT (808 nm wavelength;30 mW power output;47 seconds irradiation time;0.00785 cm² spot area;dose 180 J/cm2;irradiance 3.8 W/cm2;1.4 J total energy per point/section;and 5.6 J total energy per point per lower limb and 224 J total dose delivered over the whole protocol - 40 sessions). The authors concluded that the strength training associated with LLLT is more beneficial than training for strength. In the present study there was improvement of the grip strength in the 904 nm group when applied before strengthening.
Literature presents a large number of researches with LLLT and muscle performance. However, there is no standardization of the parameters applied, and the lack of studies about evaluation of wrist extensor muscles, and wrist and finger flexors, makes it difficult to compare the results, and to understand the mechanisms involved. Consequently, it is necessary to conduct new studies to identify the importance, and dependency between each LLLT and grip, in order to improve their specificity in development of different methodologies.
Limitations of the present study are the lack of a double-blind evaluation;follow-up time, comparison with other models, and other LLLT application;and not performing another type of analysis, such as electromyography or biomarkers. In that way, new studies with different methodologies may contribute to this area.
Conclusion
In the sample, LLLT (904 nm) associated with resistance training was effective in improving grip strength when compared to LLLT (660 nm) and isolated strength training over a 4 week period.
Conflict of interests
The authors declare that they have no conflict of interests.
Ethical considerations
This study was approved by Paulista University Research Ethics Committee, protocol number: 1133/11 CEP/ICS/Trial Number 1111979851, Brazil.
Please cite this article as follows: Barbosa R, Marcolino A, Souza V, Bertolino G, Fonseca M, Guirro R. Effect of low-level laser therapy and strength training protocol on hand grip by dynamometry. J Lasers Med Sci. 2017;8(3):112-117. doi:10.15171/jlms.2017.20.
References
- 1.Kijima Y, Viegas SF. Wrist Anatomy and Biomechanics. J Hand Surg. 2009;34A:1555–1563. doi: 10.1016/j.jhsa.2009.07.019. [DOI] [PubMed] [Google Scholar]
- 2. Pratt NE. Anatomy and Kinesiology of the Hand. In: Skirven TM, Osterman AL, Fedorczyk JM, Amadio PC, eds. Rehabilitation of the Hand and Upper Extremity. 6th ed. Philadelphia: Elsevier; 2011:1–17.
- 3.Bawa P, Chalmers GR, Jones KE, Segaard K, Walsh MI. Control of the wrist joint in humans. Eur J Appl Physiol. 2000;83:116–127. doi: 10.1007/s004210000270. [DOI] [PubMed] [Google Scholar]
- 4.Krischak A, Krasteva F, Schneider D, Gulkin F, Gebhard M. Physiotherapy after volar plating of wrist fractures is effective using a home exercise program. Arch Phys Med Rehabil. 2009;90(4):537–44. doi: 10.1016/j.apmr.2008.09.575. [DOI] [PubMed] [Google Scholar]
- 5.Bertrand AM, Fournier K, Brasey MGW, Kaiser ML, Frischknecht R, Diserens K. Reliability of maximal grip strength measurements and grip strength recovery following a stroke. J Hand Ther. 2015;28(4):356–62. doi: 10.1016/j.jht.2015.04.004. [DOI] [PubMed] [Google Scholar]
- 6.Szekeres M, MacDermid JC, King GJW, Grewal R. The relationship between the patient-rated ulnar nerve evaluation and the common impairment measures of grip strength, pinch strength, and sensation. J Hand Ther. 2014;28(1):39–45. doi: 10.1016/j.jht.2014.10.003. [DOI] [PubMed] [Google Scholar]
- 7.Karagiannopoulos C, Sitler M, Michlovitz S, Tierney R. A descriptive study on wrist and hand sensori-motor impairment and function following distal radius fracture intervention. J Hand Ther. 2013;26(3):204–215. doi: 10.1016/j.jht.2013.03.004. [DOI] [PubMed] [Google Scholar]
- 8.Johnston JA, Bobich LR, Santello M. Coordination of intrinsic and extrinsic hand muscle activity as a function of wrist joint angle during two-digit grasping. Neurosci Lett. 2010;474(2):104–108. doi: 10.1016/j.neulet.2010.03.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Gavi MB, Vassalo DV, Amaral FT. et al. Strengthening exercises improve symptoms and quality of life but do not change autonomic modulation in fibromyalgia: a randomized clinical trial. Plos One. 2014;9:e90767. doi: 10.1371/journal.pone.0090767. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Fernandes LF, Araújo MS, Matheus JP, Medalha CC, Shimano AC, Pereira GA. Comparação de Dois Protocolos de Fortalecimento para Preensão Palmar. Rev Bras Fisioterapia. 2003;7(1):17–23. [Google Scholar]
- 11.Barbosa RI, Marcolino AM, Guirro RRJ, Mazzer N, Barbieri CH, Fonseca MCR. Efeito do laser de baixa intensidade (660 nm) na lesão do nervo isquiático em ratos. Fisioterapia Pesquisa. 2010;17:294–299. [Google Scholar]
- 12.Barbosa RI, Marcolino AM, de Jesus Guirro RR, Mazzer N, Barbieri CH, de Cássia Registro Fonseca M . Comparative effects of wavelengths of low-power laser in regeneration of sciatic nerve in rats following crushing lesion. Lasers Med Sci. 2010;25(3):423–430. doi: 10.1007/s10103-009-0750-8. [DOI] [PubMed] [Google Scholar]
- 13.Batista JD, Sargenti-Neto S, Dechichi P, Rocha FS, Pagnoncelli RM. Low-level laser therapy on bone repair:is there any effect outside the irradiated field? Lasers Med Sci. 2015;30(5):1569–74. doi: 10.1007/s10103-015-1752-3. [DOI] [PubMed] [Google Scholar]
- 14.Allahverdi A, Sharifi D, Takhtfooladi MA, Hesaraki S, Khansari M, Dorbeh SS. Evaluation of low-level laser therapy, platelet-rich plasma, and their combination on the healing of Achilles tendon in rabbits. Lasers Med Sci. 2015;30(4):1305–1313. doi: 10.1007/s10103-015-1733-6. [DOI] [PubMed] [Google Scholar]
- 15.Toma RL, Tucci HT, Antunes HK. et al. Effect of 808 nm low-level laser therapy in exercise-induced skeletal muscle fatigue in elderly women. Lasers Med Sci. 2013;28(5):1375–1382. doi: 10.1007/s10103-012-1246-5. [DOI] [PubMed] [Google Scholar]
- 16.De Marchi T, Leal Junior EC, Bortoli C, Tomazoni SS, Lopes-Martins RA, Salvador M. Low-level laser therapy (LLLT) in human progressive-intensity running:effects on exercise performance, skeletal muscle status, and oxidative stress. Lasers Med Sci. 2012;27(1):231–236. doi: 10.1007/s10103-011-0955-5. [DOI] [PubMed] [Google Scholar]
- 17.Aquino AE Jr, Sene-Fiorese M, Paolillo FR. et al. Low-level laser therapy (LLLT) combined with swimming training improved the lipid profile in rats fed with high-fat diet. Laser Med Sci. 2013;28(5):1271–1280. doi: 10.1007/s10103-012-1223-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Leal-Junior ECP, Vanin AA, Miranda EF, Carvalho PTC, Corso SD, Bjordal JM. Effect of phototherapy (low-level laser therapy and light-emitting diode therapy) on exercise performance and markers of exercise recovery: a systematic review with meta-analysis. Lasers Med Sci. 2013;30(2):925–939. doi: 10.1007/s10103-1465-4,. [DOI] [PubMed] [Google Scholar]
- 19.Baroni BM, Rodrigues R, Freire BB, Franke RA, Geremia JM, Vaz MA. Effect of low-level laser therapy on muscle adaptation to knee extensor eccentric training. Eur J Appl Physiol. 2015;115:639–647. doi: 10.1007/s00421-014-3055-y. [DOI] [PubMed] [Google Scholar]
- 20.Higahi RH, Toma RL, Tucci HT. et al. Effects of low-level laser therapy on biceps brachialis muscle fatigue in young women Photomed. Laser Surg. 2013;31(12):586–594. doi: 10.1089/pho.2012.3388. [DOI] [PubMed] [Google Scholar]
- 21.Dos Reis FA1, da Silva BA, Laraia EM. et al. Effects of pre- or post-exercise low-level laser therapy (830 nm) on skeletal muscle fatigue and biochemical markers of recovery in humans: double-blind placebo-controlled trial. Photomed Laser Surg. 2014;32(2):106–112. doi: 10.1089/pho.2013.3617. [DOI] [PubMed] [Google Scholar]
- 22.Leal Junior EC, Lopes-Martins RA, Rossi RP. et al. Effect of cluster multi-diode light emitting diode therapy (LEDT) on exercise-induced skeletal muscle fatigue and skeletal muscle recovery in humans. Lasers Surg Med. 2009;41(8):572–577. doi: 10.1002/lsm.20810. [DOI] [PubMed] [Google Scholar]
- 23.Vieira WH, Ferraresi C, Perez SE, Baldissera V, Parizotto NA. Effects of low-level laser therapy (808 nm) on isokinetic muscle performance of young women submitted to endurance training: a randomized controlled clinical trial. Lasers Med Sci. 2012;27(2):497–504. doi: 10.1007/s10103-011-0984-0. [DOI] [PubMed] [Google Scholar]
- 24.Felismino AS, Costa EC, Aoki MS. et al. Effect of low-level laser therapy (808 nm) on markers of muscle damage: a randomized double-blind placebo-controlled trial. Lasers Med Sci. 2013;9(3):933–938. doi: 10.1007/s10103-013-1430-1432. [DOI] [PubMed] [Google Scholar]
- 25.Vasheghani MM, Bayat M, Dadpay M, Habibie M, Rezaei F. Low-level laser therapy using 80-Hz pulsed infrared diode laser accelerates third-degree burn healing in rat. Photomed Laser Surg. 2009;27(6):959–964. doi: 10.1089/pho.2008.2366. [DOI] [PubMed] [Google Scholar]
- 26.Mathiowetz V, Wiemer DM, Federman SM. Grip and pinch strength:norms for 6- to 19-year-olds. Am J Occup Ther. 1986;40(10):705–711. doi: 10.5014/ajot.40.10.705. [DOI] [PubMed] [Google Scholar]
- 27.Marcolino AM, Fonseca M, Colombari F, Rodrigues E, Tamanini G, Barbosa R. Influence of volar and dorsal static orthoses in different wrist positions on muscle activation and grip strength in healthy subjects. Hand Ther. 2014;19(4):114–125. [Google Scholar]
- 28.Nampo FK, Cavalheri V, Dos Santos Soares F, de Paula Ramos S, Camargo EA. Low-level phototherapy to improve exercise capacity and muscle performance:a systematic review and meta-analysis. Lasers Med Sci. 2016;31(9):1957–1970. doi: 10.1007/s10103-016-1977-9. [DOI] [PubMed] [Google Scholar]
- 29.Enwemeka CS. Standard parameters in laser phototherapy. Photomed Laser Surg. 2008;26(3):411. doi: 10.1089/pho.2008.9770. [DOI] [PubMed] [Google Scholar]
- 30.Prado R, Neves L, Marcolino A. et al. Effect of low-level laser therapy on malondialdehyde concentration in random cutaneous flap viability. Photomed Laser Surg. 2010;28(3):379–384. doi: 10.1089/pho.2009.2535. [DOI] [PubMed] [Google Scholar]
- 31.Marcolino AM, Barbosa RI, Neves LMS, Mazzer N, Guirro RRJ, Fonseca MCR. Assessment of functional recovery of sciatic nerve in rats submitted to low-level laser therapy with different fluences An experimental study: laser in functional recovery in rats. J Hand Microsurg. 2013;5(2):49–53. doi: 10.1007/s12593-013-0096-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Kelencz CA, Muñoz IS, Amorim CF, Nicolau RU. Effect of low power gallium–aluminum–arsenium noncoherent light (640 nm) on muscle activity: a clinical study. Photomed Laser Surg. 2010;28(5):647–652. doi: 10.1089/pho.2008.2467. [DOI] [PubMed] [Google Scholar]
- 33.Baroni BM, Leal Junior EC, Geremia JM, Diefenthaeler F, Vaz MA. Effect of light emitting diodes therapy (LEDT) on knee extensor muscle fatigue. Photomed Laser Surg. 2010;28(5):653–658. doi: 10.1089/pho.2009.2688. [DOI] [PubMed] [Google Scholar]
- 34.Ferraresi C, Oliveira TB, Zafalon LO. et al. Effects of low level laser therapy (808 nm) on physical strength training in humans. Lasers Med Sci. 2011;26:349–358. doi: 10.1007/s10103-010-0855-0. [DOI] [PubMed] [Google Scholar]