
Figure 1.
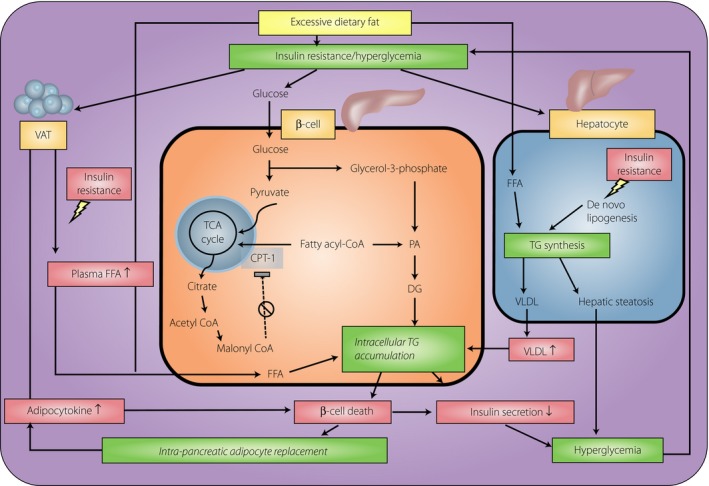
A potential interplay between dysglycemia, non‐alcoholic fatty pancreas disease (NAFPD) and β‐cell dysfunction. During long‐term intake of excessive calories, dietary fatty acids and hyperinsulinemia stimulate hepatic steatosis, leading to increased export of very‐low‐density lipoprotein (VLDL), which will increase fat delivery to the islets. In β‐cells, hyperglycemia inhibits carnitinine‐palmitoyl transferase‐1 (CPT‐1) through increasing malonyl coenzyme A (malonyl CoA), decreasing mitochondria β‐oxidation and further promoting intracellular triglyceride (TG) accumulation. In contrast, insulin resistance enhances triglyceride lipolysis and free fatty acid (FFA) release from visceral adipose tissue (VAT), thus increasing circulating FFAs. Chronic exposure of β‐cell to elevated FFAs results in increased intracellular triacylglycerol content, decreased insulin gene expression and blunted glucose‐stimulated insulin secretion. In addition, adipocyte‐derived cytokines and FFAs also contribute to β‐cell destruction, which further blunts insulin secretion as well as promotes intrapancreatic replacement by adipocytes. When fat deposition in the pancreas exceeds the tolerance threshold, hyperglycemia will supervene and causes a vicious cycle of continuous deterioration of glucometabolic state. DG, diglycerides; PA, phosphatidic acid; TCA, tricarboxylic acid.