
Figure 1.
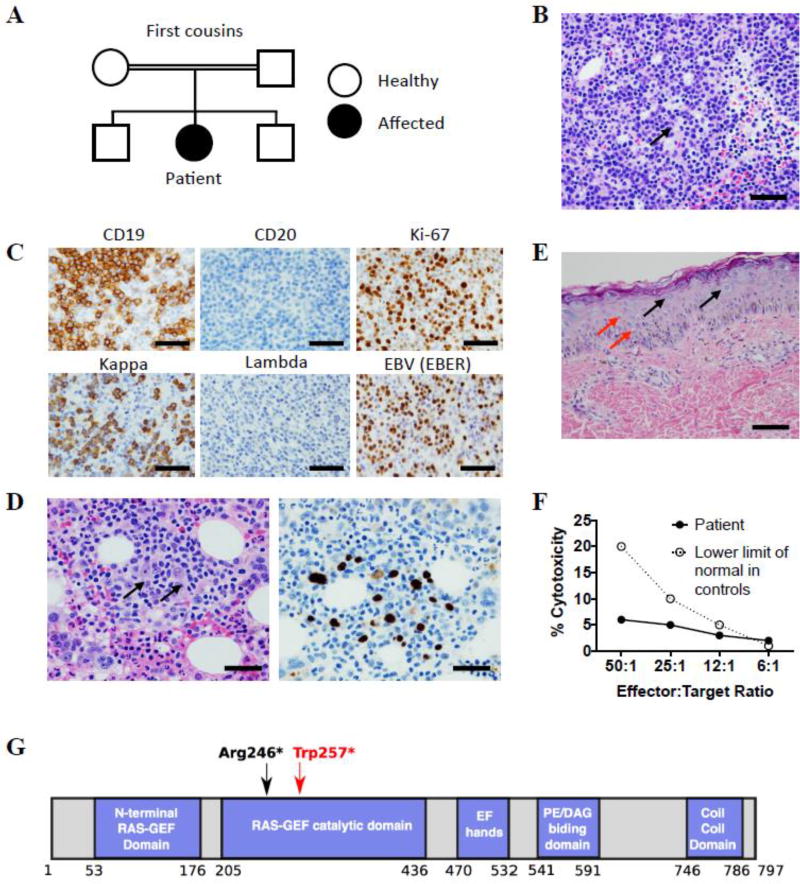
Characterization of patient phenotype. (A) Family pedigree. (B) H&E stained section of inguinal lymph node biopsy. Arrow indicates larger atypical cell, scale bar = 100 µM. (C) Inguinal lymph node biopsy: immunohistochemistry staining for CD19, CD20 and Ki-67 (top panels) and in situ hybridization for kappa, lambda and EBER (bottom panels), scale bars = 100 µM. (D) Bone marrow biopsy: H&E staining (left panel), and in situ hybridization for EBER (right panel). Arrows indicate large atypical Hodgkin-like cells, scale bars = 50 µM. (E) H&E stain of skin biopsy showing numerous large blue cells in the epidermis (black arrows) and koilocytes (red arrows), scale bar = 50 µM. (F) NK cell cytotoxicity in vitro: chromium-51 release assay using peripheral blood mononuclear cells at indicated effector to target ratios. The assay was performed in the Cincinnati Children’s Diagnostic Immunology Laboratory. (G) RASGRP1 protein domains. Red arrow indicates position of the patient’s mutation, black arrow indicates the previously reported mutation.