
Figure 2. Adipose tissue specific Raptor (mTORC1) or Rictor (mTORC2) ablation causes severe but different metabolic complications.
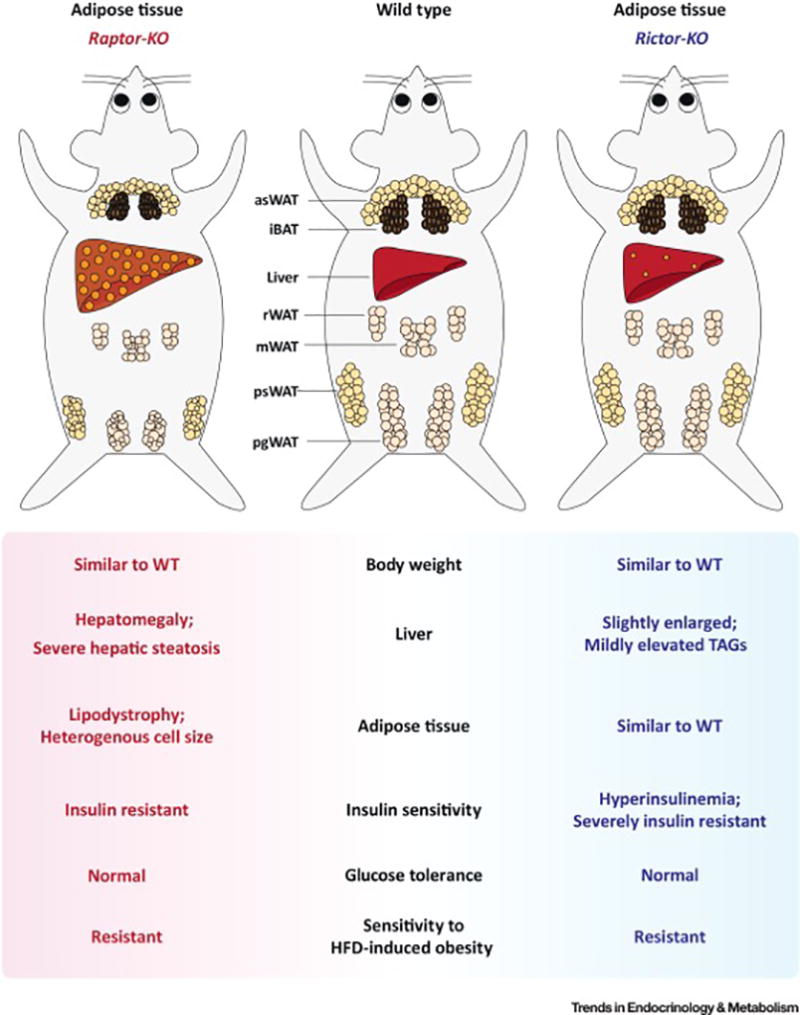
(Left) Congenital adipose tissue-specific Raptor/mTORC1 loss in mice progressively causes generalized lipodystrophy. At the cellular level, the depots are composed of heterogeneous adipocytes varying dramatically in cell size. Adipose tissue Raptor KO mice also have metabolic defects in other organs such as hepatomegaly, severe hepatic steatosis, insulin resistance, hyperphagy, and impaired gut lipid absorption.
(Right) Adipose specific Rictor/mTORC2 loss in mice has little effect on fat morphology under standard dietary conditions; however, these mice develop profound insulin resistance associated with hyperinsulinemia. These mice also have mild hepatomegaly and hepatic lipid accumulation. Moreover, their livers are insulin resistant and have elevated hepatic glucose production; however, insulin stimulated muscle glucose uptake is normal. Interestingly, both mouse models are resistant to high fat diet (HFD) induced obesity. [Abbreviations] iBAT, interscapular brown fat; asWAT, anterior subcutaneous WAT; psWAT, posterior subcutaneous WAT; mWAT, mesenteric WAT; rWAT, retroperitoneal WAT; pgWAT, perigonadal WAT.