
Figure 1.
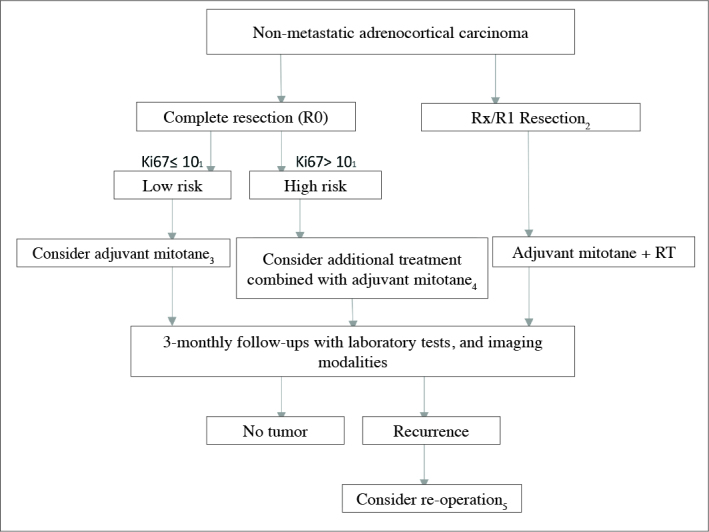
Treatment algorithm of non-metastatic adrenal carcinoma
1) If Ki67 index can not be measured, then higher proliferative index (>mitoses/5 large field) can be used in the evaluation of risk. 2) In patients who had undergone R2 resection, re-operation should be considered by an experienced surgeon. 3) Tumor diameter less than 8 cm, and lack of evidence of microscopic invasion into tumor capsule are indicators of decreased risk for recurrence.In cases which meet these conditions follow-up may be planned. 4) Individualized treatment (especially in patients who demand aggressive treatment): Ki67 ≥20, in the presence of microscopic invasion to vessels and tumor capsule decision favoring additional radiotherapy directed to tumor bed, if tumor thrombus is seen in vena cava, then decision favoring administration of additional dose of streptozotocin. 5) Re-operation is recommended if complete resection is feasible, and a time interval of less than 12 months passed between primary surgery and recurrence. If this time interval is less than 6 months, since most of the patients would not benefit from resection of the recurrent lesion, systemic treatment is initiated as soon as possible.