
Figure 8. Sirt2 deficiency blunts the cardioprotective function of metformin.
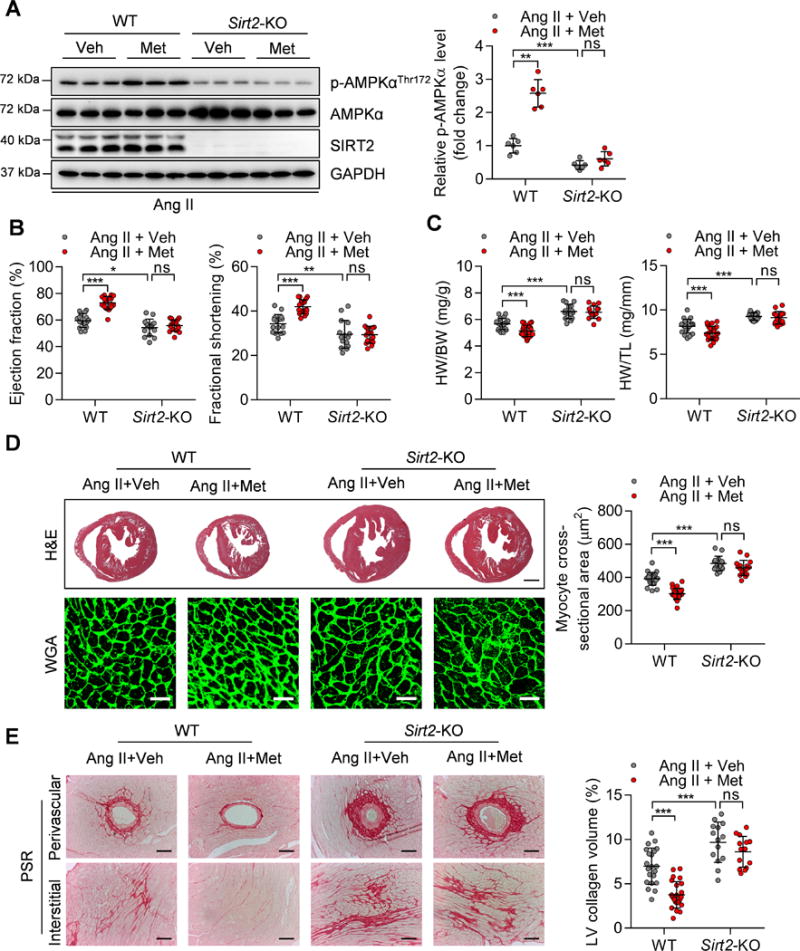
(A) Left: Representative western blotting showing the phosphorylation of AMPK at Thr172 in the hearts of WT and Sirt2-KO mice treated with Ang II (1.3 mg/kg/day) and metformin (200 mg/kg/day). Veh: Vehicle; Met: Metformin. Right: Quantification of phosphorylated AMPK levels (n=6; **P<0.01, ***P<0.001, ns: not significant).
(B) Ejection fraction and fractional shortening of WT and Sirt2-KO mice treated with Ang II and metformin (n=15~17; *P<0.05, **P<0.01, ***P<0.001, ns: not significant).
(C) Ratios of heart weight-to-body weight (HW/BW) or heart weight-to-tibia length (HW/TL) in WT and Sirt2-KO mice treated with Ang II and metformin (n=15~24; ***P<0.001, ns: not significant).
(D) Left: Hematoxylin-eosin (H&E, scale bar=1 mm) staining and wheat germ agglutinin (WGA, scale bar=30 μm) staining were performed to determine the hypertrophic growth of the hearts in WT and Sirt2-KO mice treated with Ang II and metformin. Right: Quantification of cardiomyocyte size of the hearts in WT and Sirt2-KO mice treated with Ang II and metformin (n=14~24; ***P<0.001, ns: not significant).
(E) Left: Picrosirius red (PSR, scale bar=50 μm) staining was performed to determine cardiac fibrosis of the hearts from WT and Sirt2-KO mice treated with Ang II and metformin. Right: Quantification of cardiac fibrosis of the hearts in WT and Sirt2-KO mice treated with Ang II and metformin (n=14~24; ***P<0.001, ns: not significant).