
Figure 1. Special Features of SDH-related Leukoencephalopathy.
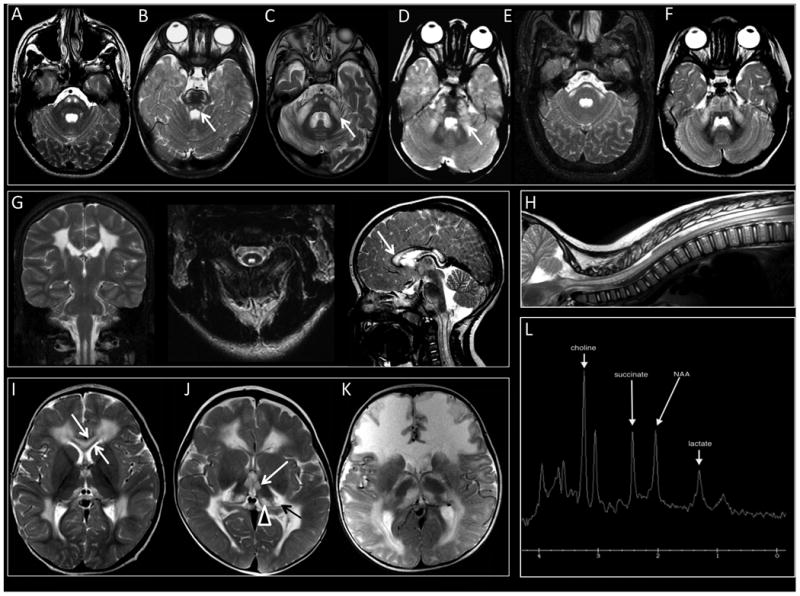
(1A) Signal abnormalities are seen in the pyramidal tracts in the pons (Image from Individual 1). (1B) The transverse pontine fibers are often affected and in a few cases, the central tegmental tracts (white arrow) (Image from Individual 13). (1C and 1D) Signal abnormalities are seen lateral portions of the middle cerebellar peduncles (Arrows, Images from Individuals 7 and 4, respectively). (1E and 1F) In some cases, a transverse band across the pons is observed with extension into the middle cerebellar peduncles (Images from Individuals 2 and 8, respectively). (1G and 1H) The dorsal portion of the cervical and sometimes also thoracic spinal cord is often affected (Images from Individual 1). The inner and outer blades are spared (white arrow). (1I and 1J) Extensive cerebral hemispheric white matter abnormalities are seen predominantly involving the frontal, parieto-occipital, and posterior temporal regions, sparing the juxtacortical fibers in all lobes (Images from Individuals 8 and 10, respectively). (1K) Diffuse abnormalities involving the juxtacortical, central and periventricular white matter may also occur (Individual 15). (1I) The inner and outer blades are spared (White Arrow), while the rest of the corpus callosum is affected (Individual 8). (1J and 1K) The thalamic nuclei anterior and medial portions of the thalamic nuclei are involved (White Arrow), as well as the medial pulvinar (Arrow Head), or medial and lateral geniculate bodies bilaterally (Black Arrow, Individual 10 (1J) and Individual 15 (1K)). (1L). Single voxel MRS (TE 35 msec) with voxel of interest placed over the mid pontine signal abnormalities. Large metabolic peak at 2.4 ppm represents marked succinate elevation. Macromolecular peak centered at 1.3 ppm is consistent with abnormal lactate.