
Figure 1.
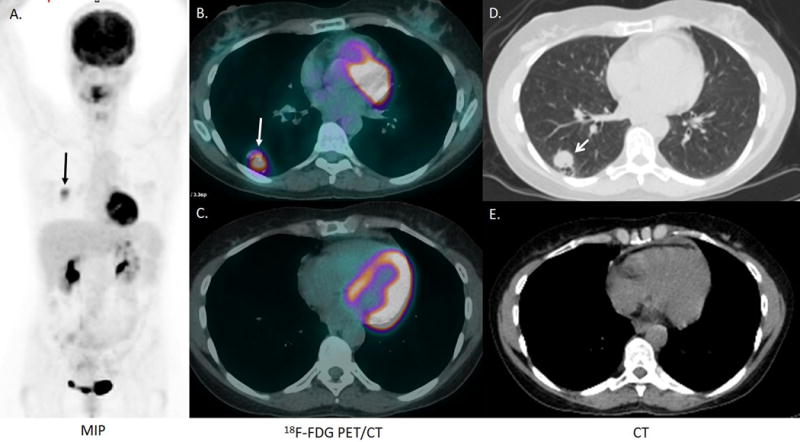
A 54-year-old woman with a history of stage IV non-small cell lung adenocarcinoma, metastatic to the mediastinum and brain, was previously treated with chemoradiation with 4 cycles of carboplatin, paclitaxel, and bevacizumab, radiation and stereotactic radiosurgery to all metastatic brain sites was in remission for 5 years. A surveillance chest CT revealed a 2.0 × 1.6 cm right lower lobe indeterminate pulmonary nodule (not shown). 18F-FDG PET/CT was performed 73 minutes after the intravenous injection of 395.9, MBq (10.7 mCi) of 18F-FDG. The MIP image (A) and the fusion and CT images (B, C) demonstrate intense FDG uptake in the 2.0 × 1.6 cm right lower lobe nodule, and physiologic intense FDG uptake in the brain and myocardium (A, B, C). Intense FDG uptake was also detected in a 1.4 × 1.5 cm left adrenal nodule and 1.7 × 2.5 cm proximal right thigh soft tissue nodule (not shown). A brain MRI demonstrated no significant changes in the appearance of the treated brain metastases, and no new brain metastases (not shown). Pathology from an excisional biopsy of the right thigh nodule revealed metastatic sarcomatoid carcinoma most compatible with a lung primary. Immunohistochemical stains demonstrated that the tumor cells were diffusely and strongly positive for cytokeratins (AE1/AE3 and CAM 5.2), while negative for S100, muscle-specific actin, smooth muscle actin, h-caldesmon, and myogenin. Genetic analysis of the tumor revealed a KRAS mutation and a BRAF V600L mutation.