
Figure 7.
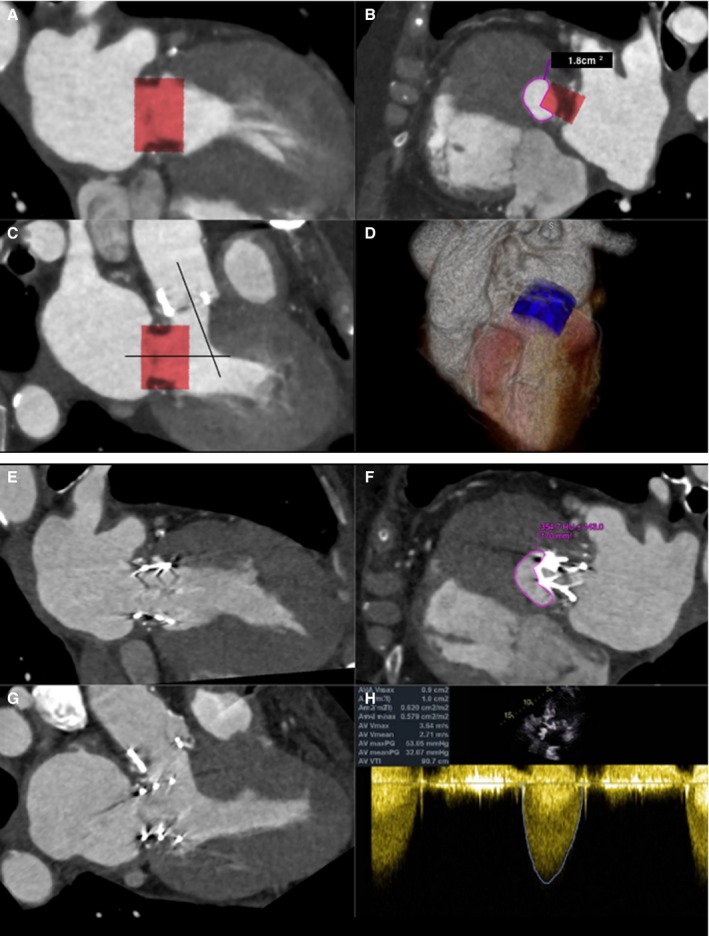
A through D, ECG gated, contrast‐enhanced cardiac computerized tomographic image (CT) at end systole showing (A) commissural and (B) 3‐chamber views with a simulated Edwards SAPIEN XT valve (26 mm) oriented perpendicularly to the annular plane of a bioprosthetic St. Jude valve (27 mm). Note the acute aortomitral angle. One third of the cylinder volume is projected to remain above the annular plane. The neo–left ventricular outflow tract (LVOT) formed by the septal myocardium and the device is shown (C) with cross‐sectional area of 1.8 cm2, indicating high risk for LVOT obstruction. D, Three‐dimensional (3D) rendering of the cylinder within the left ventricle. E through H, Contrast‐enhanced cardiac CT at end systole showing an Edwards SAPIEN XT transcatheter heart valve (26 mm) in the mitral position. Commissural (E), 3‐chamber (F), and neo‐LVOT (G) views demonstrate end‐systolic area of 1.7 cm2. A transthoracic echocardiogram (H) showed combined peak and mean gradients across the LVOT/bioprosthetic aortic valve of 53 and 32 mm Hg. Pre–transcatheter mitral valve replacement (TMVR) peak and mean gradients across the aortic valve were 37 and 13 mm Hg, respectively. The procedure, performed for early bioprosthetic valve failure and severe mitral regurgitation (MR), was clinically successful. Intraoperative transesophageal echocardiogram showed trivial MR after the deployment of the TMVR, which translated into improved symptoms.