

Abstract
Study Objectives:
There is limited information on the relationship between risk of cardiovascular disease and the joint effects of sleep quality and sleep duration, especially from large, prospective, cohort studies. This study is to prospectively investigate the joint effects of sleep quality and sleep duration on the development of coronary heart disease.
Methods:
This study examined 60,586 adults aged 40 years or older. A self-administered questionnaire was used to collect information on sleep quality and sleep duration as well as a wide range of potential confounders. Events of coronary heart disease were self-reported in subsequent medical examinations. Two types of Sleep Score (multiplicative and additive) were constructed to reflect the participants' sleep profiles, considering both sleep quality and sleep duration. The Cox regression model was used to estimate the hazard ratio (HR) and the 95% confidence interval (CI).
Results:
A total of 2,740 participants (4.5%) reported new events of coronary heart disease at follow-up. For sleep duration, participants in the group of < 6 h/d was significantly associated with an increased risk of coronary heart disease (HR: 1.13, 95% CI: 1.04–1.23). However, the association in the participants with long sleep duration (> 8 h/d) did not reach statistical significance (HR: 1.11, 95% CI: 0.98–1.26). For sleep quality, both dreamy sleep (HR: 1.21, 95% CI: 1.10–1.32) and difficult to fall asleep/use of sleeping pills or drugs (HR: 1.40, 95% CI: 1.25–1.56) were associated with an increased risk of the disease. Participants in the lowest quartile of multiplicative Sleep Score (HR: 1.31, 95% CI: 1.16–1.47) and of additive sleep score (HR: 1.31, 95% CI: 1.16–1.47) were associated with increased risk of coronary heart disease compared with those in the highest quartile.
Conclusions:
Both short sleep duration and poor sleep quality are associated with the risk of coronary heart disease. The association for long sleep duration does not reach statistical significance. Lower Sleep Score (poorer sleep profile) increases the risk of coronary heart disease, suggesting the importance of considering sleep duration and sleep quality together when developing strategies to improve sleep for cardiovascular disease prevention.
Citation:
Lao XQ, Liu X, Deng HB, Chan TC, Ho KF, Wang F, Vermeulen R, Tam T, Wong MC, Tse LA, Chang LY, Yeoh EK. Sleep quality, sleep duration, and the risk of coronary heart disease: a prospective cohort study with 60,586 adults. J Clin Sleep Med. 2018;14(1):109–117.
Keywords: cohort study, coronary heart disease, sleep duration, sleep quality, sleep score
BRIEF SUMMARY
Current Knowledge/Study Rationale: There is increasing evidence showing that short sleep duration and poor sleep quality are associated with cardiovascular disease. However, there is little information on the joint effects of quality and duration of sleep, despite the fact that a comprehensive sleep profile should consist of both.
Study Impact: We conducted a large, prospective cohort study to investigate the joint effects of quality and duration of sleep on the development of coronary heart disease. Our study substantially advances our understanding of the importance of considering sleep duration and sleep quality together when developing strategies to improve sleep for cardiovascular disease prevention.
INTRODUCTION
Cardiovascular disease is a leading cause of death and disability worldwide. The number of cardiovascular deaths is projected to increase to more than 24 million by 2030, resulting in a huge disease burden.1 Poor lifestyle and behavior are believed to be the leading causes of cardiovascular disease.2 Sleep, which is a basic human behavior, is reported to be associated with the risk of cardiovascular disease and other health outcomes.3–5
A comprehensive sleep profile includes sleep duration and sleep quality. Getting enough quality sleep is important for maintaining cardiovascular health. However, most previous studies focused on sleep duration. A growing number of studies have demonstrated that short sleep duration increases the risk of cardiovascular disease.6–11 A few studies have also shown that poor sleep quality was associated with higher risk of cardiovascular disease.8–13 Some researchers have argued that sleep quality is more important than sleep duration.14,15 However, there are limited data about the joint effects of sleep quality and sleep duration on the risk of cardiovascular disease, especially from large, prospective cohort studies. People spend one-third of their lifetime asleep. Approximately one-third of the general population regularly suffers from sleep-related problems, and this figure has increased in recent years.16 We therefore conducted a large, prospective cohort study to investigate sleep and coronary heart disease while taking into account the effects of both sleep duration and sleep quality.
METHODS
Setting and Participants
The current data analysis was based on the prospective cohort study of 590,977 Taiwan residents between 1996 and 2014. The cohort details have been described elsewhere.17,18 Briefly, the participants joined a standard medical examination program provided by a private firm (MJ Health Management Institution, Taipei, Taiwan). Each participant received a series of medical examinations including a general physical examination and biochemical tests of blood and urine, as well as a standard self-administered questionnaire survey. A total of 256,980 participants regularly visited the firm twice or more. Because cardiovascular events generally occur in middle-aged and older people, we restricted our analysis to those participants aged 40 years or older. We also excluded those who reported the following physician-diagnosed diseases in the first visit: cardiovascular disease (including coronary heart disease, peripheral arterial disease, rheumatic heart disease, congenital heart disease, deep vein thrombosis, and pulmonary embolism), cerebrovascular diseases, diabetes, thyroid disease, tuberculosis, asthma, chronic obstructive pulmonary disease, peptic ulcer, hepatitis and liver cirrhosis, chronic kidney disease, and cancer. Finally, we analyzed 60,586 participants aged 40 years or older. Details of the participant selection are presented in Figure S1 in the supplemental material. Each participant gave written informed consent when they joined the MJ Health Screening Program authorizing MJ Health Management Institution to process data generated from the medical examination program. Personal identification was removed and remained anonymous when the data were released for this research. We obtained ethical approval for the current study from the Joint Chinese University of Hong Kong – New Territories East Cluster Clinical Research Ethics Committee.
Ascertainment of the Outcome
The health outcome used in the current study was incident of coronary heart disease. Baseline information was retrieved from the first visit of each participant. The end point was either a subsequent visit in which the participant first reported a diagnosis by a physician of a new coronary heart disease event or the final visit if the participant did not receive a diagnosis of coronary heart disease. To collect the information, the participants were asked: “Were you ever diagnosed as having a coronary heart disease by a physician?” Those participants who answered “yes” on their second visit onward were then defined as having a new event of coronary heart disease.
Sleep Assessment
Participants were asked two questions to assess their sleep duration and sleep quality in the visit. For sleep duration, they were asked “How many hours do you usually sleep a day?” with the following four answer options: < 4 hours, 4–6 hours, 6–8 hours, and > 8 hours. Because only a small number of participants slept fewer than 4 h/d, these participants were grouped with those who slept for 4 to 6 h/d when we assessed the association between sleep duration and the risk of coronary heart disease.
For sleep quality, participants were asked “How did you evaluate your sleep situation last month?” with the following answer options: use of sleeping pills or drugs, difficult to fall asleep, dreamy sleep, can fall asleep but easily awaken, and sleep well. Because the number of participants reporting use of sleeping pills or drugs was very small, this group was combined with those who found it difficult to fall asleep when we assessed the association between sleep quality and the risk of coronary heart disease.
Potential Confounders
Information on potential confounders collected in the baseline was used in the current data analysis, including: education (primary school or below, middle school, college, and university or above), marital status (single, married, divorced, and widowed), family history of cardiovascular disease (yes, no), alcohol drinking (never, former, and current), cigarette smoking (never, former, and current), physical exercise in leisure time (light, moderate, high, and vigorous), physical activity in work (sedentary job, job requiring approximately half sedentary and half walking, job mostly requiring walking and standing, and job requiring vigorous physical activity), fruit intake (< 1 and ≥ 1 servings/d), and vegetables intake (< 0.5, 0.5 to < 1.0, and ≥ 1.0 bowls/d). Weight and height were measured using an autoanthropometer (Nakamura KN-5000A, Tokyo, Japan) with the participants barefoot and wearing light clothes to calculate body mass index. Diastolic and systolic blood pressures were measured using a computerized auto-mercury sphygmomanometer (Citizen CH-5000, Tokyo, Japan). Total cholesterol (mg/dl), fasting glucose (mg/dl), and triglyceride level (mg/dl) were measured using the Hitachi 7150 autoanalyzer (Hitachi ltd., Tokyo, Japan).19
Statistical Analysis
All analyses were conducted using R-software (version 3.2.5, The R Foundation, Vienna, Austria). P values were derived from two-sided statistical tests and a value of P < .05 was considered to be statistically significant.
We constructed two types of Sleep Score by combining sleep duration and quality for data analysis. We assigned a score to each category of sleep duration and sleep quality for calculating the Sleep Score (ie, for sleep quality, we assigned the numbers 5, 4, 3, 2, and 1 to the categories of “sleep well”, “can fall asleep but easily awake,” “dreamy sleep,” “difficult to fall asleep,” and “use of sleeping pills or drugs,” respectively; for sleep duration: we assigned the numbers 4, 3, 2, and 1 to the categories of 6–8 h/d, > 8 h/d, 4–6 h/d, and < 4 h/d, respectively). The Sleep Score was used to reflect the whole sleep profile (ie, a higher Sleep Score reflects a better sleep profile). The following formula was applied for the multiplicative Sleep Score calculation:
where the Sleep Score (multiplicative) ranged from 1 to 20. The following formula was applied for the additive Sleep Score calculation:
where the Sleep Score (additive) ranged from 2 to 9. The Sleep Score distributions are presented in Figure 1.
Figure 1. Distribution of the Sleep Score.
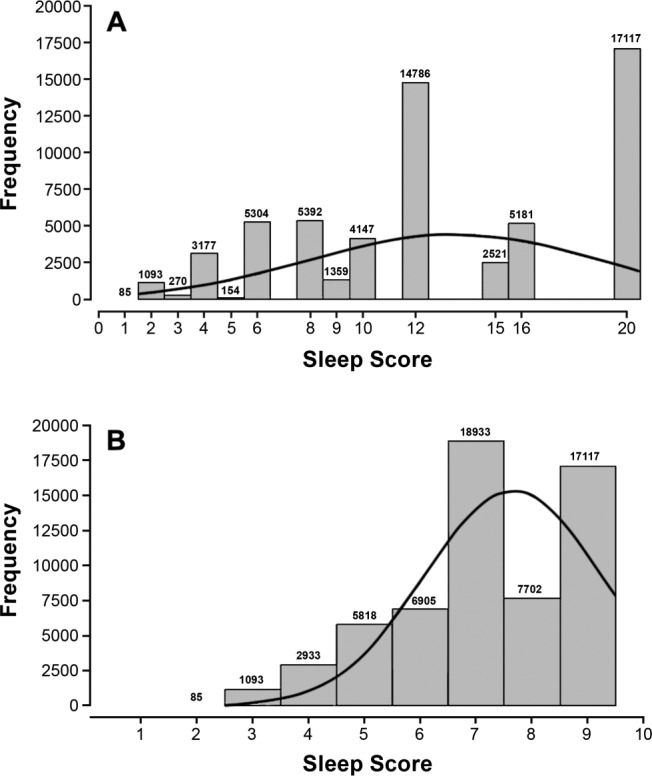
(A) Histogram of Sleep Score (multiplicative) in the participants. (B) Histogram of Sleep Score (additive) in the participants.
Unadjusted and adjusted hazard ratio (HR) with 95% confidence intervals (95% CI) was estimated using Cox regression models to assess the association between sleep and the risk of coronary heart disease. We assessed the associations between coronary heart disease and sleep duration, sleep quality, and Sleep Score separately. We also categorized the participants into quartiles with respect to their Sleep Score and compared the risk between different quartiles. To remove potential modification effects from sex and age, we conducted subgroup analysis by stratifying the sex and age groups (40– 60 years and > 60 years). We also conducted the following sensitivity analyses for comparison: (1) excluding those participants with follow-up time less than 2 years because we believed the effect of sleep on heart disease is chronic, (2) excluding those participants aged 75 years or older to avoid survival effects in the elderly, (3) excluding those participants with a family history of cardiovascular diseases to remove the confounding effect, and (4) excluding those participants in whom other diseases (including hypertension, cerebrovascular diseases, diabetes, thyroid disease, tuberculosis, asthma, peptic ulcer, hepatitis and liver cirrhosis, nephritis and cancer) developed during the follow-up, because these diseases may have intermediate effects.
RESULTS
A total of 60,586 participants aged 40 years or older were included in the analysis. Table 1 presents the baseline characteristics of the participants. The mean (standard deviation) of age, body mass index, and follow-up period were 50.6 (8.6) years, 23.8 (3.2) kg/m2, and 5.6 (4.4) years, respectively. No significant difference was observed in age and follow-up duration between sex (P > .1).
Table 1.
Baseline characteristics of the participants.

During the follow-up, a total of 2,740 participants (4.52%) reported having coronary heart disease. Among the participants, no significant difference was observed in the cumulative incidence of disease between sex (male versus female: 4.59% versus 4.46%, P = .447). The cumulative incidence of coronary heart disease increased from 2.1% in the participants aged 40 to 45 years to 12.0% in the participants aged 71 to 75 years and then decreased to 9.7% in the participants aged 75 years or older. Similar trends were observed in males and females (Table S1 in the supplemental material).
Table 2 shows the associations between sleep and risk of coronary disease. A higher Sleep Score (multiplicative) significantly decreased the risk of coronary heart disease (every 5-unit increment of Sleep Score was associated with a 9% decrease in the risk [HR: 0.91, 95% CI: 0.88–0.94]) after fully adjusting for confounders. Compared with quartile IV of the Sleep Score, a significant higher risk of coronary heart disease was observed in quartile II (HR: 1.24, 95% CI: 1.10–1.39) and quartile I (HR: 1.31, 95% CI: 1.16–1.47). Significant exposure-response relationships were also observed (P < .001). Similar results were observed when the Sleep Score (additive) was used in separate analysis.
Table 2.
Association between sleep and risk of coronary heart disease in Taiwan residents.
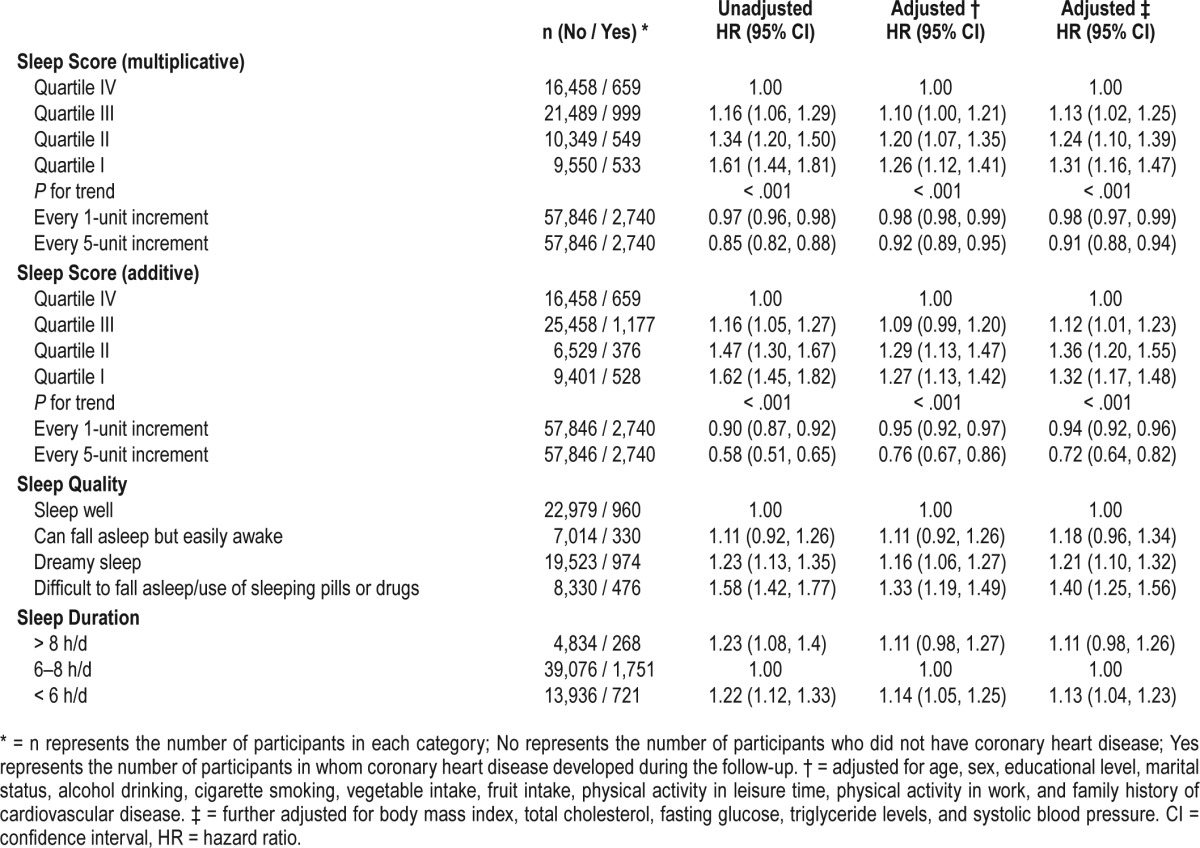
When we assessed the relationship with sleep quality and duration separately, a significant higher risk of coronary heart disease was observed in participants with dreamy sleep (HR: 1.21, 95% CI: 1.10–1.32) and difficult to fall asleep/use of sleeping pills or drugs (HR: 1.40, 95% CI: 1.25–1.56). Short sleep duration (< 6 h/d) significantly increased the risk (HR: 1.13, 95% CI: 1.04–1.23), whereas long sleep duration did not reach statistical significance (HR: 1.11, 95% CI: 0.98–1.26) (Table 2).
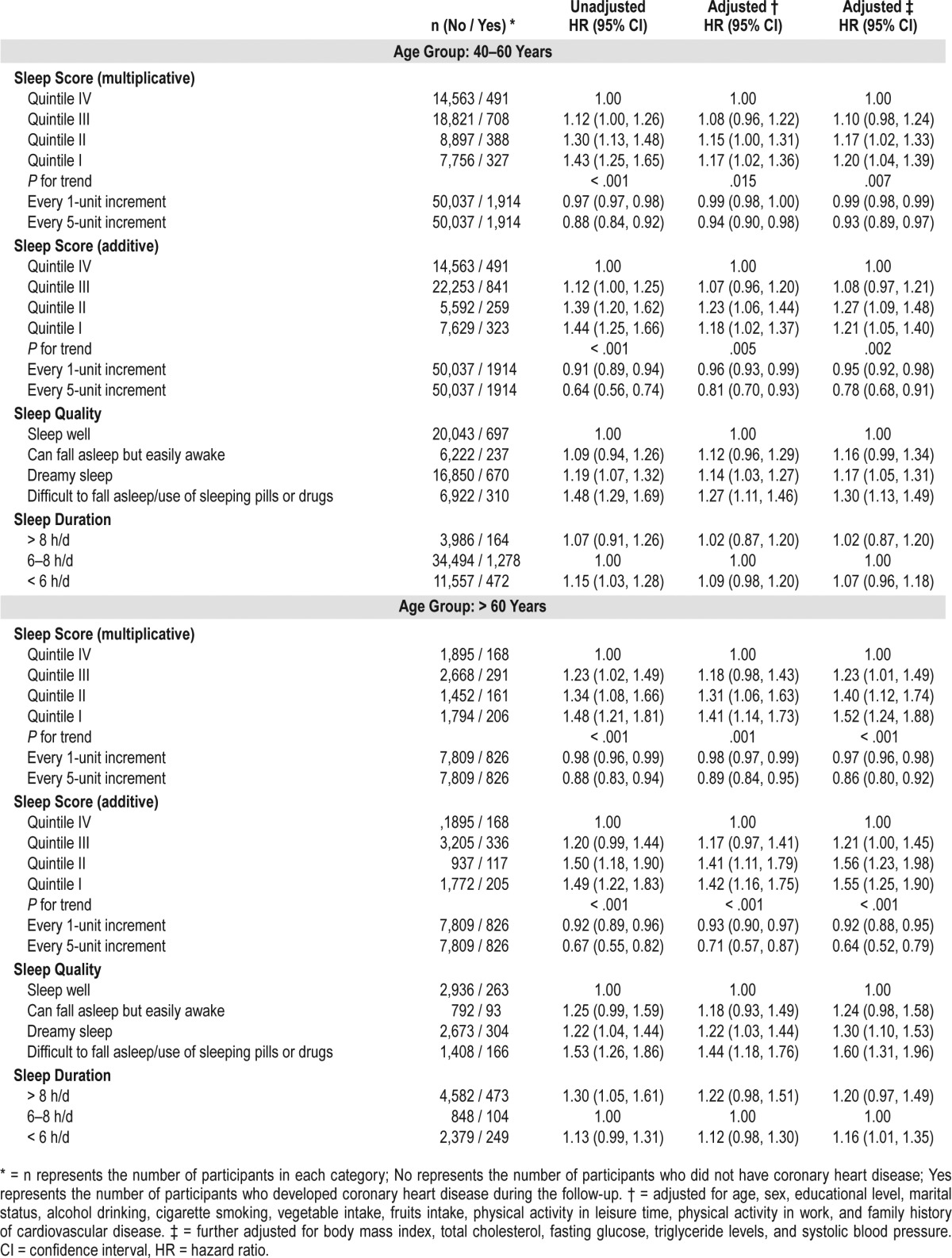
Subgroup analysis stratified by sex (Table 3) and age group (Table 4) yielded similar results. Similar results were observed in the series of sensitivity analyses: (1) excluding participants with follow-up duration less than 2 years (Table S2 in the supplemental material), (2) excluding participants aged 75 years or older (Table S3 in the supplemental material), (3) excluding participants who had family history of coronary heart disease (Table S4 in the supplemental material), and (5) excluding participants in whom other diseases developed during the follow-up (Table S5 in the supplemental material).
Table 3.
Association between sleep and risk of coronary heart disease in Taiwan residents stratified by sex.
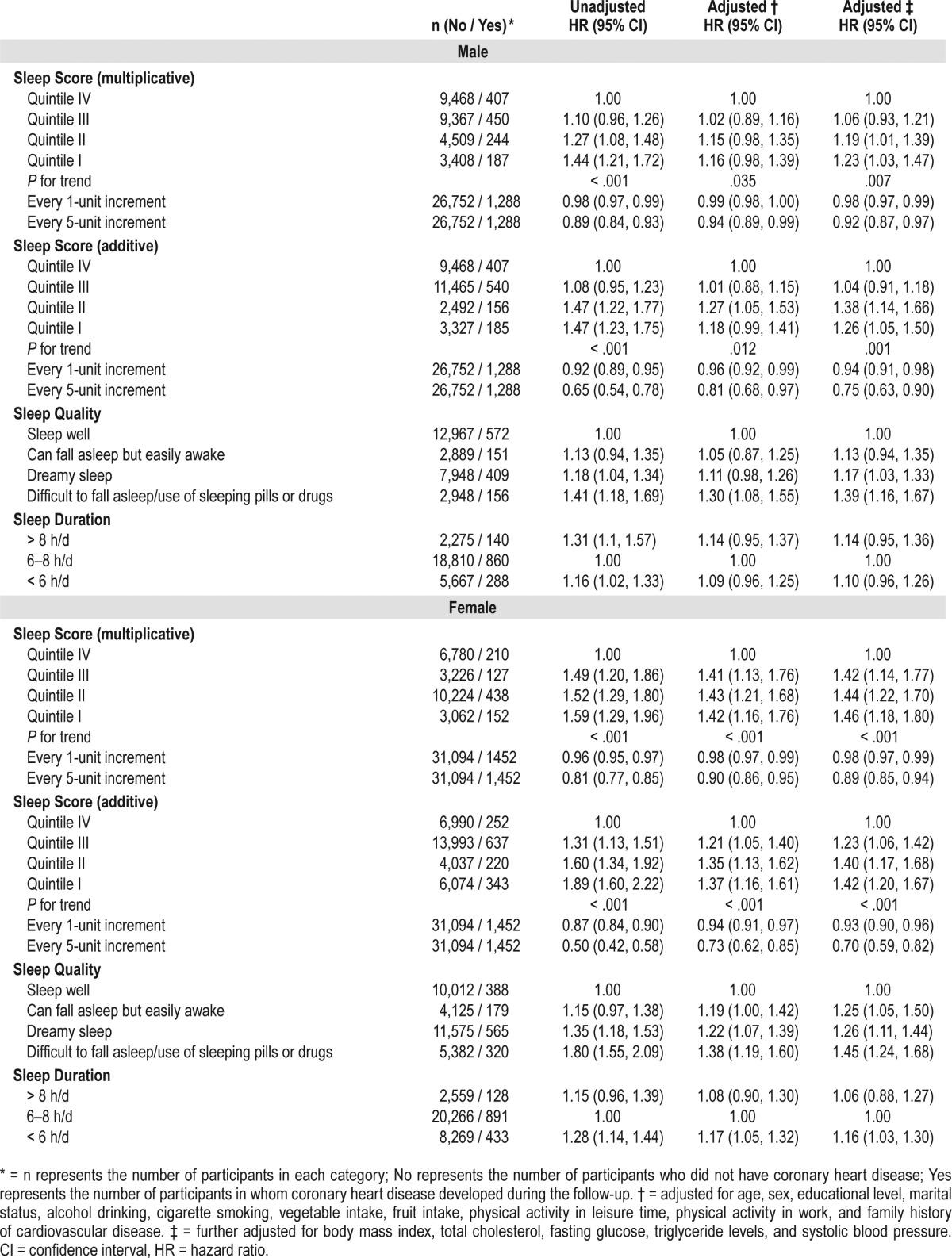
Table 4.
Association between sleep and the risk of coronary heart disease in the Taiwan residents stratified by age group.
DISCUSSION
This is the first cohort study to investigate the association between sleep and incidence of coronary heart disease by taking both sleep duration and sleep quality into consideration in a large Asian population. Our study found that both poor sleep quality and short sleep duration are independently associated with the risk of coronary heart disease events in adults aged 40 years or older. The Sleep Score, which reflects the joint effects of sleep quality and sleep duration, is significantly associated with the risk of coronary heart disease. Because sleep is a modifiable risk factor, our results suggest the importance of considering sleep duration and sleep quality together when developing strategies to improve sleep for cardiovascular disease prevention.
Previous studies have shown that short sleep duration increases the risk of cardiovascular diseases, which is consistent with the results of our study.6–11 However, the effects of long sleep duration remain uncertain, although a systematic review reported that sleep for more than 8 h/d was associated with an increased risk of coronary heart disease.20 Our study also found the association did not reach statistical significance for long sleep duration. Further studies are warranted on this topic. Poor sleep quality has also been reported to be associated with higher risk of cardiovascular diseases. The Mexican Teacher Cohort found that poor sleep quality was associated with subclinical cardiovascular disease.13 The Swedish study by Asplund shows that nightmares were associated with an increased risk in irregular heartbeat and spasmodic chest pain in elderly people.21 Studies have also reported that insomnia,22–24 difficulty falling asleep,10,25 and the use of sleeping pills26 were related to an increased risk of cardiovascular disease. Although different methods were used for evaluating sleep quality, our results are in line with the results in the findings in previous literature.
However, there are limited data on the relationship between the risk of cardiovascular disease and the joint effects of sleep quality and sleep duration, especially from large prospective cohort studies. In the current study, we constructed the Sleep Score by taking into account the effects of both sleep quality and sleep duration. We found that a lower Sleep Score (poor sleep profile) is associated with higher risk of coronary heart disease. We observed a good exposure-response relationship between the Sleep Score and the risk of coronary heart disease. The results from our study are consistent with those of previous studies using other sleep profile parameters such as the Pittsburgh Sleep Quality Index27–29 and other indicators.8,12 Neither Abraham30 nor Everding et al.31 found a significant association between sleep and cardiovascular risk factor using the Pittsburgh Sleep Quality Index. This might have been due to the young population (aged between 18–25 years) recruited in Abraham's study30 or the cross-sectional design in the study by Everding et al.31
There are several hypothesized mechanisms of the adverse effects of sleep disorders on cardiovascular health. One possible explanation is that poor sleep causes reciprocal changes in circulating levels of leptin and ghrelin,32,33 which can facilitate the development of obesity33 and impair glycemic control34 due to behavioral changes such as increasing food and calorie intake and reducing energy expenditure.35 Increased cortisol secretion and growth hormone metabolism alteration caused by sleep disorders is another hypothesis.36,37 Additionally, short sleep may trigger low-grade inflammation and lead to an increase in stress response in the hypothalamic-pituitary-adrenal axis, which may result in elevated blood pressure, interrupted blood flow, and increased risk of cardiovascular disease.38–40
This study has some important strengths. We constructed a Sleep Score to reflect the joint effects of sleep quality and sleep duration, whereas most previous studies have focused on the effects of either sleep quality or sleep duration. We also have a large sample size and cohort design, which enable us to produce stable and precise estimations. Finally, we collected comprehensive information on potential confounders and modifiers. Because poor sleep is highly correlated with poor health, it is difficult to ascertain whether poor sleep is a determinant of cardiometabolic disease or a sign of comorbid conditions without excluding participants with preexisting diseases and taking the metabolic risk factors into account. In the current study, we conducted a series of subgroup/sensitivity analyses and they yielded similar results.
However, there are several limitations to our approach. First, information on sleep duration and sleep quality was collected from the questionnaire, which is similar to most other epidemiological studies. However, it is not practical to measure sleep quality by equipment in a large-scale study. Previous studies show that when self-reported total sleep has been compared with sleep diaries, actigraphy, and polysomnography, there has generally been a good correlation between self-reported and objective measurements.41,42 Second, information on change of the sleep profile was not able to be taken into account. Sleep duration and sleep quality might be changed during follow-up for some participants. Third, our health outcomes were self-reported. However, this should not affect our conclusion, because coronary heart disease is a serious condition for which patients generally seek medical examination and treatment from their physicians. Fourth, we did not take sleep apnea into account. This might have led us to underestimate the effects of sleep quality. Fifth, positive family history is a major risk factor for coronary artery disease; however, these data are not available in this study. Finally, the construction of the Sleep Score was quite subjective. We assigned a value to each category of duration and quality. Although we were quite sure about the rank order of the categories, we were not sure whether the differences between the categories were proportionally equal. No signifi-cant interaction effects were observed between duration and quality of sleep (P = .072). Nonetheless, we used both multiplicative and additive Sleep Scores for comparison, and both yielded the same directions.
CONCLUSIONS
In conclusion, both short sleep duration and poor sleep quality are associated with the risk of coronary heart disease. The association for long sleep duration remains uncertain. A poorer sleep profile (including sleep duration and sleep quality) increases the risk of coronary heart disease in adults aged 40 years or older. Our findings suggest the importance of considering sleep duration and sleep quality together when developing strategies to improve sleep for cardiovascular disease prevention.
DISCLOSURE STATEMENT
Any interpretation or conclusion described in this paper does not represent the views of MJ Health Research Foundation. This study was partially supported by the Environmental Health Research Fund of the Chinese University of Hong Kong (No. 7104946; PI: Dr. Lao Xiang Qian). The funders had no role in the study design, data collection, analysis and interpretation, writing of the report, or the decision to submit the article for publication. All authors approved the final version of the manuscript. The authors report no conflicts of interest.
ACKNOWLEDGMENTS
The authors thank MJ Health Research Foundation for authorizing us to use the MJ health data (Authorization code: MJHR2015002A). Author contributions: XQL conceptualized and designed this study; XDL analyzed the data; XDL and XQL drafted the manuscript and interpreted the results; other co-authors reviewed the manuscript and were involved in results interpretation. All co-authors provided critical comments and approved the final version.
ABBREVIATIONS
- CI
confidence interval
- HR
hazard ratio
REFERENCES
- 1.Fuster V, Kelly BB, Vedanthan R. Promoting global cardiovascular health: moving forward. Circulation. 2011;123(15):1671–1678. doi: 10.1161/CIRCULATIONAHA.110.009522. [DOI] [PubMed] [Google Scholar]
- 2.Writing Group Members. Mozaffarian D, Benjamin EJ, Go AS, et al. Heart Disease and Stroke Statistics-2016 Update: A Report From the American Heart Association. Circulation. 2016;133(4):E38–E360. doi: 10.1161/CIR.0000000000000350. [DOI] [PubMed] [Google Scholar]
- 3.Lee SW, Ng KY, Chin WK. The impact of sleep amount and sleep quality on glycemic control in type 2 diabetes: A systematic review and meta-analysis. Sleep Med Rev. 2017;31:91–101. doi: 10.1016/j.smrv.2016.02.001. [DOI] [PubMed] [Google Scholar]
- 4.Howell D, Oliver TK, Keller-Olaman S, et al. Sleep disturbance in adults with cancer: a systematic review of evidence for best practices in assessment and management for clinical practice. Ann Oncol. 2014;25(4):791–800. doi: 10.1093/annonc/mdt506. [DOI] [PubMed] [Google Scholar]
- 5.Covassin N, Singh P. Sleep duration and cardiovascular disease risk: epidemiologic and experimental evidence. Sleep Med Clin. 2016;11(1):81–89. doi: 10.1016/j.jsmc.2015.10.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Magee CA, Kritharides L, Attia J, McElduff P, Banks E. Short and long sleep duration are associated with prevalent cardiovascular disease in Australian adults. J Sleep Res. 2012;21(4):441–447. doi: 10.1111/j.1365-2869.2011.00993.x. [DOI] [PubMed] [Google Scholar]
- 7.Ayas NT, White DP, Manson JE, et al. A prospective study of sleep duration and coronary heart disease in women. Arch Intern Med. 2003;163(2):205–209. doi: 10.1001/archinte.163.2.205. [DOI] [PubMed] [Google Scholar]
- 8.Hoevenaar-Blom MP, Spijkerman AM, Kromhout D, van den Berg JF, Verschuren WM. Sleep duration and sleep quality in relation to 12-year cardiovascular disease incidence: the MORGEN study. Sleep. 2011;34(11):1487–1492. doi: 10.5665/sleep.1382. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Westerlund A, Bellocco R, Sundstrom J, Adami HO, Akerstedt T, Trolle Lagerros Y. Sleep characteristics and cardiovascular events in a large Swedish cohort. Eur J Epidemiol. 2013;28(6):463–473. doi: 10.1007/s10654-013-9802-2. [DOI] [PubMed] [Google Scholar]
- 10.Sabanayagam C, Shankar A, Buchwald D, Goins RT. Insomnia symptoms and cardiovascular disease among older American Indians: the Native Elder Care Study. J Environ Public Health. 2011;2011:964617. doi: 10.1155/2011/964617. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Chandola T, Ferrie JE, Perski A, Akbaraly T, Marmot MG. The effect of short sleep duration on coronary heart disease risk is greatest among those with sleep disturbance: a prospective study from the Whitehall II cohort. Sleep. 2010;33(6):739–744. doi: 10.1093/sleep/33.6.739. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Twig G, Shina A, Afek A, et al. Sleep quality and risk of diabetes and coronary artery disease among young men. Acta Diabetol. 2016;53(2):261–270. doi: 10.1007/s00592-015-0779-z. [DOI] [PubMed] [Google Scholar]
- 13.Merino P, Catzín-Kuhlmann A, Monge A, et al. Sleep quality is associated with subclinical cardiovascular disease in mid-life Mexican women [abstract] Circulation. 2017;135(suppl 1):AMP087. [Google Scholar]
- 14.Bin YS. Is sleep quality more important than sleep duration for public health? Sleep. 2016;39(9):1629–1630. doi: 10.5665/sleep.6078. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Yang TC, Park K. To what extent do sleep quality and duration mediate the effect of perceived discrimination on health? Evidence from Philadelphia. J Urban Health. 2015;92(6):1024–1037. doi: 10.1007/s11524-015-9986-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Roth T. Insomnia: definition, prevalence, etiology, and consequences. J Clin Sleep Med. 2007;3(5 Suppl):S7–S10. [PMC free article] [PubMed] [Google Scholar]
- 17.Wen CP, Cheng TY, Tsai MK, et al. All-cause mortality attributable to chronic kidney disease: a prospective cohort study based on 462 293 adults in Taiwan. Lancet. 2008;371(9631):2173–2182. doi: 10.1016/S0140-6736(08)60952-6. [DOI] [PubMed] [Google Scholar]
- 18.Chang SS, Wen CP, Tsai MK, Lawlor DA, Yang YC, Gunnell D. Adiposity, its related biologic risk factors, and suicide: a cohort study of 542,088 Taiwanese adults. Am J Epidemiol. 2012;175(8):804–815. doi: 10.1093/aje/kwr386. [DOI] [PubMed] [Google Scholar]
- 19.Strand LB, Tsai MK, Gunnell D, Janszky I, Wen CP, Chang SS. Self-reported sleep duration and coronary heart disease mortality: a large cohort study of 400,000 Taiwanese adults. Int J Cardiol. 2016;207:246–251. doi: 10.1016/j.ijcard.2016.01.044. [DOI] [PubMed] [Google Scholar]
- 20.Itani O, Jike M, Watanabe N, Kaneita Y. Short sleep duration and health outcomes: a systematic review, meta-analysis, and meta-regression. Sleep Med. 2017;32:246–256. doi: 10.1016/j.sleep.2016.08.006. [DOI] [PubMed] [Google Scholar]
- 21.Asplund R. Nightmares, sleep and cardiac symptoms in the elderly. Neth J Med. 2003;61(7):257–261. [PubMed] [Google Scholar]
- 22.Canivet C, Nilsson PM, Lindeberg SI, Karasek R, Ostergren PO. Insomnia increases risk for cardiovascular events in women and in men with low socioeconomic status: a longitudinal, register-based study. J Psychosom Res. 2014;76(4):292–299. doi: 10.1016/j.jpsychores.2014.02.001. [DOI] [PubMed] [Google Scholar]
- 23.Meng L, Zheng Y, Hui R. The relationship of sleep duration and insomnia to risk of hypertension incidence: a meta-analysis of prospective cohort studies. Hypertens Res. 2013;36(11):985–995. doi: 10.1038/hr.2013.70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Silva-Costa A, Griep RH, Rotenberg L. Disentangling the effects of insomnia and night work on cardiovascular diseases: a study in nursing professionals. Braz J Med Biol Res. 2015;48(2):120–127. doi: 10.1590/1414-431X20143965. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Grandner MA, Jackson NJ, Pak VM, Gehrman PR. Sleep disturbance is associated with cardiovascular and metabolic disorders. J Sleep Res. 2012;21(4):427–433. doi: 10.1111/j.1365-2869.2011.00990.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Setoguchi M, Noda M, Ichikawa K, Usui M, Isobe M. Sleeping pills increase the risk of cardiovascular events in heart failure patients with preserved ejection fraction [abstract] Eur J Heart Fail. 2014;16(suppl 2):96–97. [Google Scholar]
- 27.Bidulescu A, Din-Dzietham R, Coverson DL, et al. Interaction of sleep quality and psychosocial stress on obesity in African Americans: the Cardiovascular Health Epidemiology Study (CHES) BMC Public Health. 2010;10:581. doi: 10.1186/1471-2458-10-581. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Meng LL, Tang YZ, Ni CL, et al. Impact of inflammatory markers on the relationship between sleep quality and incident cardiovascular events in type 2 diabetes. J Diabetes Complications. 2015;29(7):882–886. doi: 10.1016/j.jdiacomp.2015.06.011. [DOI] [PubMed] [Google Scholar]
- 29.Sharma M, Sawhney JP, Panda S. Sleep quality and duration - potentially modifiable risk factors for Coronary Artery Disease? Indian Heart J. 2014;66(6):565–568. doi: 10.1016/j.ihj.2014.10.412. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Abraham C. The Effect of Sleep Quality and High Intensity Physical Activity on Inflammation and Cardiovascular Disease Risk Factors in College Students [honors scholar theses] Storrs, CT: University of Connecticut - Storrs; 2016. [Google Scholar]
- 31.Everding B, Hallam JE, Kohut ML, Lee DC, Anderson AA, Franke WD. Association of sleep quality with cardiovascular disease risk and mental health in law enforcement officers. J Occup Environ Med. 2016;58(8):e281–e286. doi: 10.1097/JOM.0000000000000814. [DOI] [PubMed] [Google Scholar]
- 32.Spiegel K, Leproult R, L'Hermite-Baleriaux M, Copinschi G, Penev PD, Van Cauter E. Leptin levels are dependent on sleep duration: relationships with sympathovagal balance, carbohydrate regulation, cortisol, and thyrotropin. J Clin Endocrinol Metab. 2004;89(11):5762–5771. doi: 10.1210/jc.2004-1003. [DOI] [PubMed] [Google Scholar]
- 33.Taheri S, Lin L, Austin D, Young T, Mignot E. Short sleep duration is associated with reduced leptin, elevated ghrelin, and increased body mass index. PLoS Med. 2004;1(3):e62. doi: 10.1371/journal.pmed.0010062. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Schultes B, Schmid S, Peters A, Born J, Fehm HL. Sleep loss and the development of diabetes: a review of current evidence. Exp Clin Endocrinol Diabetes. 2005;113(10):563–567. doi: 10.1055/s-2005-872944. [DOI] [PubMed] [Google Scholar]
- 35.Spiegel K, Tasali E, Leproult R, Van Cauter E. Effects of poor and short sleep on glucose metabolism and obesity risk. Nat Rev Endocrinol. 2009;5(5):253–261. doi: 10.1038/nrendo.2009.23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Whitworth JA, Williamson PM, Mangos G, Kelly JJ. Cardiovascular consequences of cortisol excess. Vasc Health Risk Manag. 2005;1(4):291–299. doi: 10.2147/vhrm.2005.1.4.291. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Isgaard J. Cardiovascular disease and risk factors: the role of growth hormone. Horm Res. 2004;62(Suppl 4):31–38. doi: 10.1159/000080906. [DOI] [PubMed] [Google Scholar]
- 38.de Rooij SR, Nijpels G, Nilsson PM, et al. Low-grade chronic inflammation in the relationship between insulin sensitivity and cardiovascular disease (RISC) population associations with insulin resistance and cardiometabolic risk profile. Diabetes Care. 2009;32(7):1295–1301. doi: 10.2337/dc08-1795. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Buckley TM, Schatzberg AF. On the interactions of the hypothalamic-pituitary-adrenal (HPA) axis and sleep: normal HPA axis activity and circadian rhythm, exemplary sleep disorders. J Clin Endocrinol Metab. 2005;90(5):3106–3114. doi: 10.1210/jc.2004-1056. [DOI] [PubMed] [Google Scholar]
- 40.Meier-Ewert HK, Ridker PM, Rifai N, et al. Effect of sleep loss on C-reactive protein, an inflammatory marker of cardiovascular risk. J Am Coll Cardiol. 2004;43(4):678–683. doi: 10.1016/j.jacc.2003.07.050. [DOI] [PubMed] [Google Scholar]
- 41.Lauderdale DS, Knutson KL, Yan LL, Liu K, Rathouz PJ. Self-reported and measured sleep duration: how similar are they? Epidemiology. 2008;19(6):838–845. doi: 10.1097/EDE.0b013e318187a7b0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Silva GE, Goodwin JL, Sherrill DL, et al. Relationship between reported and measured sleep times: the Sleep Heart Health Study (SHHS) J Clin Sleep Med. 2007;3(6):622–630. [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.