

Abstract
Objective
Femoral arterial cannulation is associated with a significant risk of lower limb ischemia. The aim of the study was to assess the pressure and flow in the femoral artery using a novel bidirectional femoral cannula in a sheep model of peripheral cardiopulmonary bypass.
Methods
Peripheral cardiopulmonary bypass was established using a multistage venous cannula inserted into the internal jugular vein and the bidirectional or a conventional arterial cannula into the femoral artery in seven adult ewes. Systemic and distal perfusion pressures and flow rates were measured during cardiopulmonary bypass with flow rates of 1, 2, 3, and 4 L/min. Lower limb venous oxygen saturation and lactate levels were also measured.
Results
A significantly higher blood flow in the lower limb using the bidirectional cannula was observed and compared with a conventional cannula at all flow rates (mean flow 115 mL/min vs 10 mL/min, P < 0.05). The mean distal perfusion pressure was also significantly higher in the bidirectional cannula group (86 mm Hg vs 45 mm Hg at 4 L/min of flow, P < 0.05). The bidirectional cannula was associated with higher venous oxygen saturations in the lower limb than in the conventional cannula group; however, lower limb lactate production was similar in the two groups.
Conclusions
This in vivo data demonstrates superior distal flow and pressure characteristics of a novel bidirectional cannula compared with a conventional femoral cannula during peripheral cardiopulmonary bypass.
Key Words: Bidirectional cannula, Cardiopulmonary bypass, Leg ischemia, Peripheral cannulation
Peripheral cannulation using the femoral artery for arterial inflow is often required for complex aortic surgery or cardiac surgical procedures using minimally invasive approaches. It is also used for prolonged cardiopulmonary support with extracorporeal membrane oxygenation. A significant risk of lower limb ischemic complications after prolonged femoral arterial cannulation has been reported in the literature. Hendrickson and Glower1 reported an incidence of 11.5% after peripheral cardiopulmonary bypass (CPB). Extracorporeal membrane oxygenation support is associated with lower limb ischemic complication rates as high as 26%.2,3 The size of the femoral cannula required to maintain a patient on adequate CPB support is often the same diameter as the patient's own femoral artery, and there is little room around the cannula for distal limb perfusion. Viability of the limb is dependent on collateral blood flow, which, if poor, can cause limb ischemia resulting in a requirement for fasciotomy or worse amputation. A number of techniques have been proposed to prevent this potentially devastating complication, including the use of an end-to-side femoral artery graft4,5 or a downstream femoral perfusion catheter.1,6–8 These techniques, however, are often cumbersome to perform and are not always reliable. They are also associated with bleeding complications and an increased risk of infection. They have, therefore, not been routinely adopted. Currently, there are no simple and effective methods for ensuring adequate lower limb perfusion during femoral cannulation for CPB. There is a clinical need for a new type of femoral cannula that will deliver standard retrograde perfusion without compromising distal limb blood flow. We propose that this novel bidirectional femoral arterial cannula design will significantly improve perfusion to the lower limb and reduce the risk of lower limb ischemia complications during peripheral CPB.
METHODS
Design of the Bidirectional Cannula
The design of the novel bidirectional cannula is illustrated in Figure 1. The cannula is similar to a standard cannula except that it has an angled shoulder with a side hole for distal limb perfusion. It is circumferentially tapered to minimize leak during insertion. The angled shoulder provides tactile feedback to ensure correct positioning (Fig. 2). The size of the downstream perfusion port has been calibrated to provide approximately 7% of total perfusion to the lower limb.
FIGURE 1.
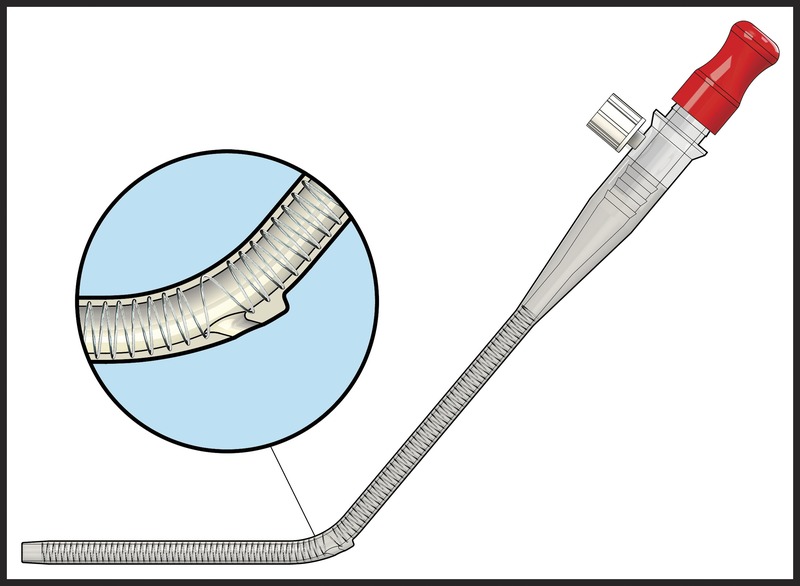
Design of the bidirectional cannula. The aperture in the shoulder of the cannula provides blood flow to the lower limb.
FIGURE 2.
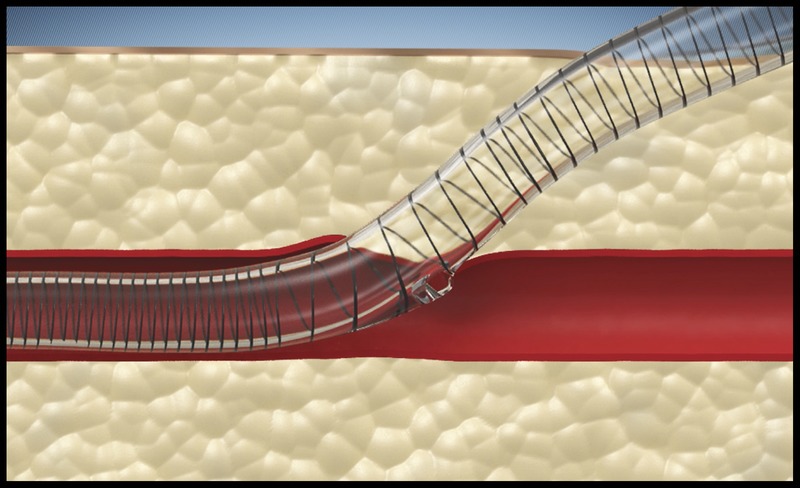
Position of bidirectional cannula within femoral artery.
Animals and General Experimental Details
All experiments were conducted in accordance with the National Health and Medical Research Council of Australia Code of Practice for the Care of Animals for Scientific Purposes (2004) and were approved by the Monash Health Animal Ethics Committee.
The study was conducted between February and April 2011. Seven adult ewes weighing approximately 60 kg were used in the study. Sheep of this size have about the same circulating blood volume as adult humans and the femoral artery caliber is similar to adult human size, allowing the insertion of cannula sizes ranging from 16F to 20F.
Peripheral CPB
Using 6 mg/kg propofol induction and 2% isoflurane maintenance, the ewes were anesthetized and placed in the supine position. An arterial cannula (20G) was inserted into the carotid artery using a cutdown technique for pressure monitoring. A multistage venous cannula was inserted into the jugular vein with the tip sitting inside the right atrium and secured with a purse-string suture. The femoral arteries were exposed by surgical cutdown and the anterior wall of the femoral artery was dissected bilaterally. One side was randomly chosen for the bidirectional cannula and the contralateral side for a standard femoral arterial cannula (Optisite arterial cannula; Edwards Lifesciences Corp, Irvine, CA USA). An ultrasound flow probe was applied to the femoral artery 2 to 3 cm distal to the insertion point of the cannula to measure flow downstream of the cannula, and a pressure monitoring cannula was inserted into the femoral artery 4- to 6-cm downstream. Cardiopulmonary bypass was established using 1 L of crystalloid priming solution. Flow was increased in 1-L increments from 1 to 4 L. Measurements of distal pressure and flow were taken at each flow rate after a 20-minute period of stabilization. The heart lung machine consisted of a venous reservoir, roller pump and membrane oxygenator connected by nonheparin-coated tubing. Femoral venous oxygen saturation and lactate levels were measured on both sides at each data collection point.
The insertion technique of the bidirectional cannula was similar to the standard cannula. A purse-string suture was placed in the front wall of the femoral artery. Using a Seldinger technique, a guide wire was passed through the purse-string suture into the femoral artery and the puncture site progressively dilated. The cannula was inserted until the shoulder of the cannula was inside the vessel lumen then pulled back until resistance was felt indicating correct positioning of the shoulder and downstream perfusion port.
Removal of the bidirectional cannula was performed by stabilizing the distal femoral artery behind the cannula insertion point and providing gentle upward traction on the cannula to deliver the cannula shoulder out of the artery.
Statistical Analysis
Data are expressed as mean ± SE of the mean. Student t test was used for comparing means between two groups of continuous data. A P value 0.05 or less was considered statistically significant. Prism 5 (GraphPad Software Inc, San Diego, CA USA) was used for graphing and statistical analysis.
RESULTS
The mean ± SE femoral artery diameter was 7 ± 0.04 mm. The 18F cannulae were chosen for both the bidirectional and the standard cannulae. No technical difficulties were encountered inserting the standard or bidirectional cannulae. Adequate systemic pressures were achieved on bypass with both the standard and bidirectional cannulae. The standard cannulae resulted in very poor distal femoral perfusion. In contrast, there was up to 130 mL/min distal flow through the bidirectional cannulae (Fig. 3). The corresponding distal perfusion pressure was also higher in the bidirectional cannula group (Fig. 4).
FIGURE 3.
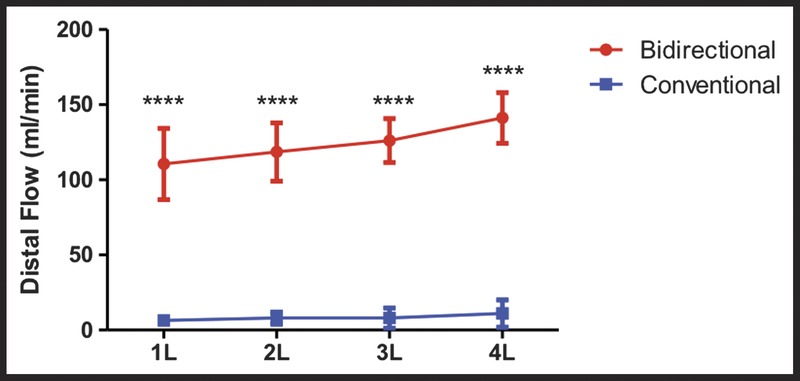
Flow in distal superficial femoral artery using bidirectional or conventional cannula (N = 7 in each group). ****P < 0.001.
FIGURE 4.
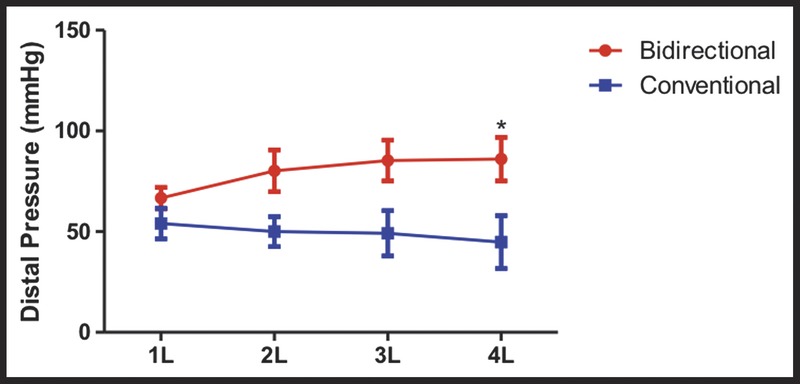
Pressure in distal superficial femoral artery using bidirectional or conventional cannula (N = 7 in each group). *P < 0.05.
Venous saturation in the limb was significantly lower in the standard cannula side compared with the bidirectional cannula side (Fig. 5). Because of the short duration of each study, a statistically significant difference in lactate production in the two groups was not seen (Fig. 6). No difficulties were encounter with removal of the bidirectional cannula.
FIGURE 5.
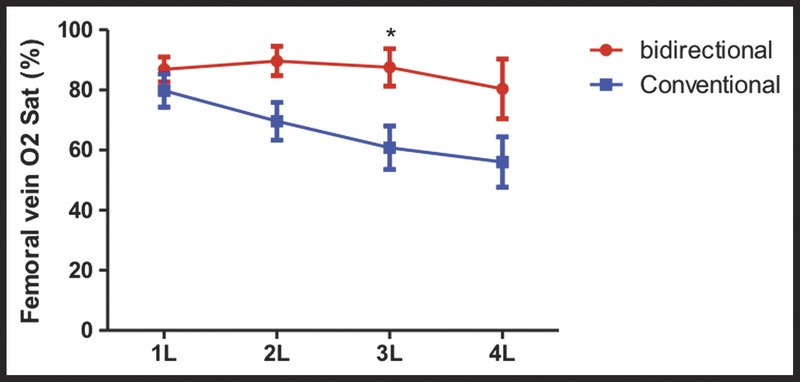
Femoral vein oxygen saturation in bidirectional and conventional cannula groups (N = 7 in each group). *P < 0.05.
FIGURE 6.
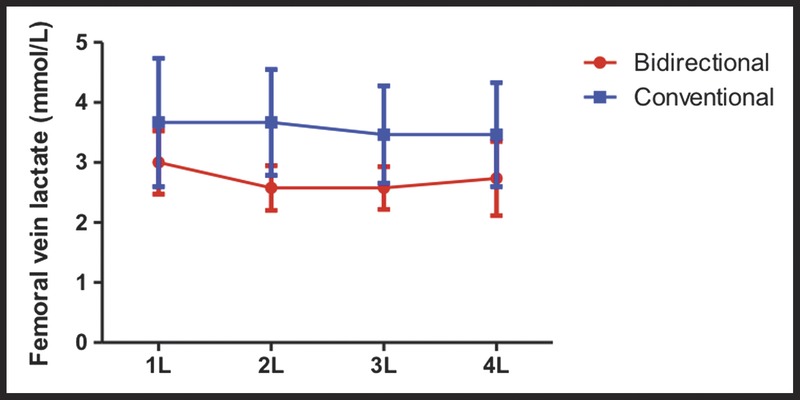
Femoral vein lactate levels in bidirectional and conventional cannula groups (N = 7 in each group).
DISCUSSION
In this study, we have demonstrated the feasibility of using a novel bidirectional femoral cannula in a sheep model of peripheral CPB to provide distal limb perfusion. The novel bidirectional cannula was simple to insert and position, was hemostatic, and demonstrated good distal flow and pressure characteristics. The bidirectional cannula was able to provide up to 150 mL/min of blood flow downstream. In an average adult, the blood flow through the superficial femoral artery is approximately 150 mL/min.6 Thus, the bidirectional cannula would be able to supply adequate blood flow to the lower limb at full CPB support.
Previously, a number of studies have investigated bidirectional cannulae.9–11 The distal-flow cannula designed by Magovern et al10 has a diverting side hole with two supporting rails on either side. The side hole sits on the under surface of the cannula and flow would be directed toward the back wall of the artery. The rails may also cause trauma to the vessel during insertion. The cannula reported by Matsui et al11 required ultrasound confirmation for positioning and risks dislodgement of the side hole into the subcutaneous tissues with movement.
The bidirectional cannula design evaluated in this study does not rely on ultrasound for positioning. Flow through the second aperture is directed downstream rather than toward the back wall of the artery. The tapered shoulder allows for atraumatic insertion, provides tactile feedback during positioning, and prevents dislodgement of the side hole into the subcutaneous tissues.
In conclusion, we have demonstrated superior femoral artery flow and pressure characteristics of a novel bidirectional femoral cannula compared with a standard femoral cannula. A commercial version of this novel bidirectional femoral cannula (Sorin Group USA, a wholly owned subsidiary of LivaNova PLC, Arvada, CO USA) is currently being evaluated in a phase 1 clinical trial at the Alfred Hospital in Melbourne, Australia.
CLINICAL PERSPECTIVE
This in vivo study fromDr Chen and colleagues from Monash University assessed the performance of a novel bidirectional femoral cannula in a sheep model of cardiopulmonary bypass (CPB). Peripheral CPB was established using a multistaged venous cannula inserted into the internal jugular vein and either a bidirectional or a conventional arterial cannula into the femoral artery. Significantly higher blood flow in the lower extremity was seen when comparing animals that were cannulated with the bidirectional versus the conventional cannula at all CPB flow rates. The use of the bidirectional cannula was also associated with higher mean distal perfusion pressures and higher venous oxygen saturations. Although lower extremity lactate production was statistically similar in both groups, lactate production was lower in the bidirectional group, and the lack of difference may have been due to the small numbers of experimental animals.
This is a well-designed and well-performed experimental study that clearly demonstrated the benefits of this bidirectional femoral cannula. The results from the phase I clinical trial will be keenly anticipated. This study suggests that this cannula may have significant benefits in both minimally invasive valve and other cardiac surgical patients undergoing peripheral cannulation.
Footnotes
Disclosures: Randall A. Moshinsky, FRACS, Elli Tutungi, FANZCA, and James McMillan, CCP, have a commercial relationship with LivaNova, London, United Kingdom. Yi Chen, FRACS, Sara M. Tayeh, CCP, Jess K. Underwood, CCP, Adam C. Wells, CCP, and Julian A. Smith, FRACS, declare no conflicts of interest.
REFERENCES
- 1.Hendrickson SC, Glower DD. A method for perfusion of the leg during cardiopulmonary bypass via femoral cannulation. Ann Thorac Surg. 1998;65:1807–1808. [DOI] [PubMed] [Google Scholar]
- 2.Foley PJ, Morris RJ, Woo EY, et al. Limb ischemia during femoral cannulation for cardiopulmonary support. J Vasc Surg. 2010;52:850–853. [DOI] [PubMed] [Google Scholar]
- 3.Huang SC, Yu HY, Ko WJ, et al. Pressure criterion for placement of distal perfusion catheter to prevent limb ischemia during adult extracorporeal life support. J Thorac Cardiovasc Surg. 2004;128:776–777. [DOI] [PubMed] [Google Scholar]
- 4.Satta J, Rimpilainen J, Rainio P, et al. A feasible femoral cannulation method during cardiopulmonary bypass. Ann Thorac Surg. 1998;65:1194–1195. [DOI] [PubMed] [Google Scholar]
- 5.Vander Salm TJ. Prevention of lower extremity ischemia during cardiopulmonary bypass via femoral cannulation. Ann Thorac Surg. 1997;63:251–252. [DOI] [PubMed] [Google Scholar]
- 6.Greason KL, Hemp JR, Maxwell JM, Fetter JE, Moreno-Cabral RJ. Prevention of distal limb ischemia during cardiopulmonary support via femoral cannulation. Ann Thorac Surg. 1995;60:209–210. [PubMed] [Google Scholar]
- 7.Kasirajan V, Simmons I, King J, Shumaker MD, DeAnda A, Higgins RS. Technique to prevent limb ischemia during peripheral cannulation for extracorporeal membrane oxygenation. Perfusion. 2002;17:427–428. [DOI] [PubMed] [Google Scholar]
- 8.Yoshimura N, Ataka K, Nakagiri K, et al. A simple technique for the prevention of lower limb ischemia during femoral veno-arterial cardiopulmonary support. J Cardiovasc Surg (Torino). 1996;37:557–559. [PubMed] [Google Scholar]
- 9.Berdajs D, Ferrari E, Michalis A, et al. New prototype of femoral arterial SmartCannula with anterograde and retrograde flow. Perfusion. 2011;26:271–275. [DOI] [PubMed] [Google Scholar]
- 10.Magovern JA, Fonger JD, Wang DH, et al. A femoral artery cannula that allows distal blood flow. J Thorac Cardiovasc Surg. 2005;130:684–686. [DOI] [PubMed] [Google Scholar]
- 11.Matsui Y, Shimura S, Suto Y, Fukase S, Tanaka A, Sasaki S. A novel femoral arterial cannula to prevent limb ischemia during cardiopulmonary support: preliminary report of experimental and clinical experiences. Artif Organs. 2006;30:557–560. [DOI] [PubMed] [Google Scholar]