
Figure 2.
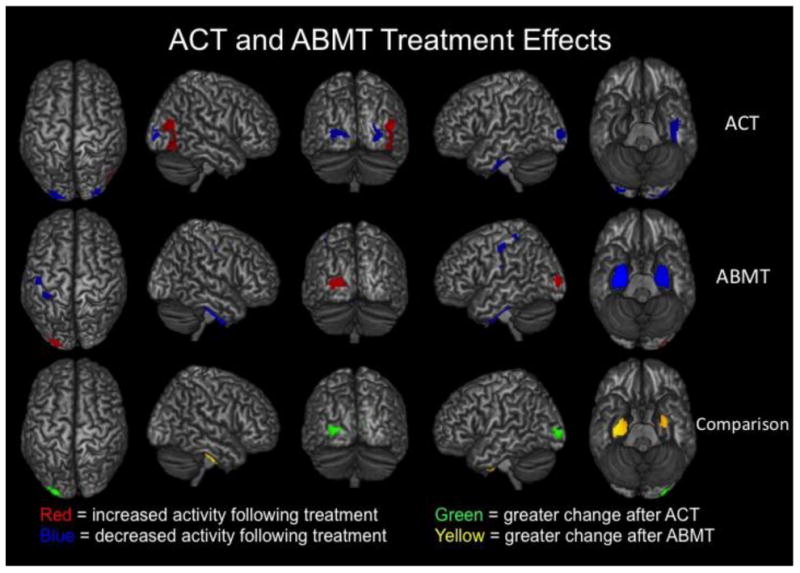
Both ACT and ABMT reduced PTSD symptoms and modulated neuronal activity during the resting-state, but the two therapies affected largely distinct brain regions. In the top two rows, brain regions that exhibited significantly (p < 0.01, corrected) increased activity following therapy are shown in red, whereas those with significantly (p <0 .01, corrected) decreased activity following therapy are shown in blue. Results for pre- to post-ACT appear in the top row and those for pre- to post- ABMT are directly below in the middle row. As shown, ACT tended to modulate posterior and lateral occipital regions, as well as left medial temporal areas (p <0.01, corrected). In contrast, ABMT affected sensorimotor, left posterior occipital, and a large volume of tissue in bilateral medial temporal regions including the amygdalae and parahippocampal complex (p <0 .01, corrected). The two therapies also exerted significantly different effects in some brain regions, and these are shown in the bottom row. First, differential images were created for each treatment (pre-treatment – post-treatment) and the a two-sample t-test was conducted. Note that that pretreatment differences were probed between groups and none were detected. This two-sample t-test showed that ABMT decreased neuronal activity in bilateral medial temporal regions significantly more than ACT, while ACT modulated occipital activity significantly more strongly than ABMT (p < 0.01, corrected).