
Figure 3.
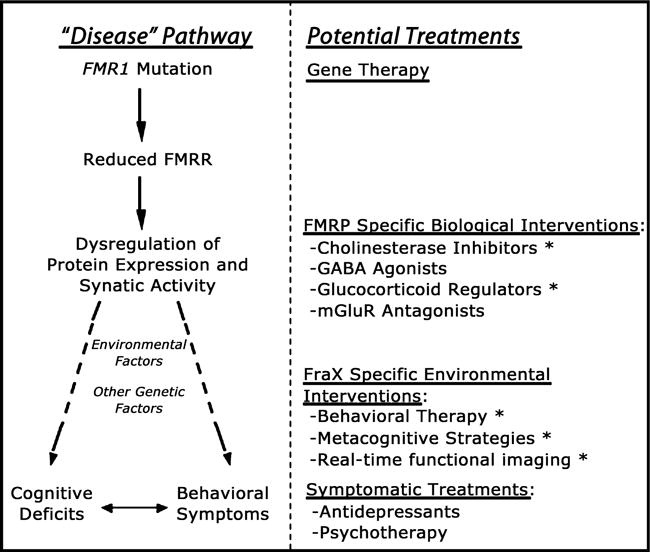
A hierarchical model for planning treatment strategies in fragile X syndrome. The left-hand side of the diagram shows the genetic and neurobiological mechanisms leading to brain dysfunction in this condition. Specifically, the FMR1 mutation causes reduction in FMRP, leading to transcriptional dysregulation of FMRP mRNA targets (involved in synapse maturation and function). Other (non-FMR1 related) genetic and environmental factors interact with this genetic-neurobiological pathway, ultimately culminating in the cognitive-behavioral phenotype associated with fragile X. The right-hand side of the diagram shows potential treatment approaches matched to the corresponding genetic and pathophysiological level on the left. Given that gene therapy approaches are not feasible at the present time, the most promising current approaches are at the level of pathways ‘downstream’ to reduced levels of FMRP (shown under the category of ‘FMRP-specific Biological Interventions). Abbreviations: FraX: fragile X syndrome; FMRP: fragile X mental retardation protein; mGlurR: metabotropic glutamate receptor; GABA: gammaaminobutyric acid. Asterisks (*) next to treatment approaches indicate ongoing trials in the Center for Interdisciplinary Brain Sciences Research at Stanford University