
Figure 2.
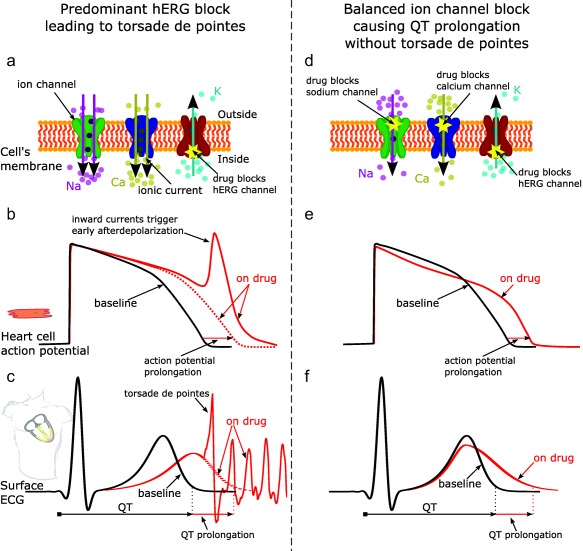
Effect of predominant hERG potassium channel block vs. balanced ion channel block on QT prolongation and generation of torsade de pointes. Illustration of predominant hERG block leading to torsade de pointes (left column) vs. balanced ion channel block causing QT prolongation without torsade de pointes (right column). Predominant hERG block reduces the hERG potassium channel current (panel a), which delays repolarization and prolongs the action potential duration of cardiomyocytes (panel b, red dotted line) and the QT interval on the ECG (panel c, red dotted line). Prolonged repolarization can result in early afterdepolarizations (panel b, red solid line), which are caused by inward currents through sodium and calcium channels11 (panel a, purple and yellow arrows) and can trigger torsade de pointes (panel c, solid red line). In addition to causing hERG block, balanced ion channel‐blocking drugs block the L‐type calcium and/or late sodium currents (panel d). While balanced ion channel block can prolong both the action potential duration of cadiomyocytes (panel e) and the QT interval on the ECG (panel f), the block of inward currents (calcium, late sodium) prevents the occurrence of early afterdepolarizations and has antiarrhythmic effects.11, 12, 13, 14, 15, 16, 17, 18 In addition, balanced ion channel block causes different morphology changes in the action potential (panel e, red solid line) and the ECG (panel f, red solid line) than predominant hERG block (panels b and c, respectively). The goal of the CiPA phase I ECG validation study described in this article is to show that exposure–response ECG analysis can differentiate predominant hERG‐blocking drugs from balanced ion channel‐blocking drugs. Na, sodium ions; Ca, calcium ions; K, potassium ions.