
Figure 1. Adjusted Prevalence of Marijuana Use Among 279 457 Pregnant Females in KPNC by Screening Type, 2009–2016.
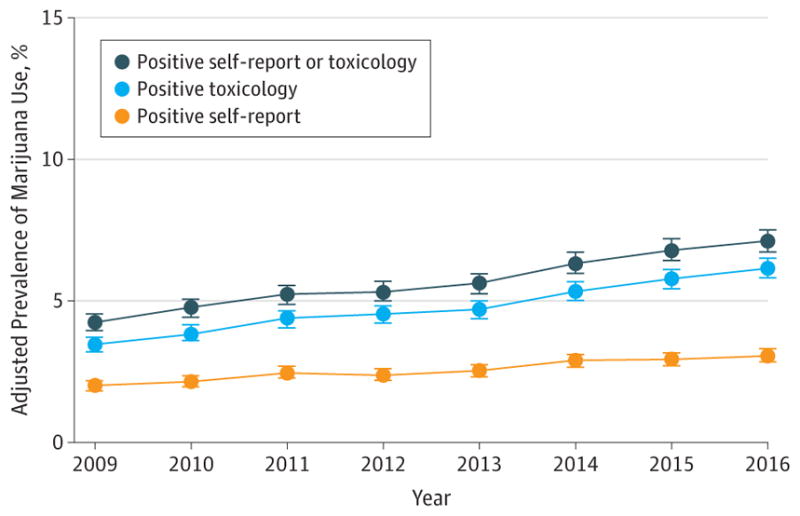
KPNC indicates Kaiser Permanente Northern California. Error bars indicate 95% CIs of the adjusted prevalences. Poisson regression models controlled for age group, race/ethnicity, and median neighborhood household income (extracted from the electronic health record). The self-reported use questionnaire and toxicology screening were part of standard prenatal care (at approximately 8 weeks’ gestation; 84%of females completed both screenings during their first trimester). For toxicology tests, 58%were completed at the same visit as the self-reported use questionnaire, 87%were completed within 14 days of completing the questionnaire, and 100% were completed within 8 weeks of completing the questionnaire. All toxicology tests were confirmed with a confirmatory laboratory test. Among pregnant females with a positive test result for prenatal marijuana use, 15.9% were positive on self-report only, 54.9%were positive on toxicology only, and 29.2%were positive on both self-report and toxicology. The sample of females included in the study was generally representative of the population of all pregnant females. There were only small differences in the demographic characteristics of females who were included vs excluded (due to missing data on prenatal marijuana use), indicating minimal to no selection bias. The median sample size across years was 34 322 (range, 32 813–38 919).