

Abstract
Objective
The primary objective of this study was to analyze the characteristics and outcomes of cases admitted to hospital with cauda equina syndrome (CES) at the Institute of Orthopedics and Traumatology (IOT) from 2005 to 2015. Secondly, this article is a continuation of the epidemiological work of the same base published in 2013, and will be important for other comparative studies to a greater understanding of the disease and its epidemiology.
Methods
This was a retrospective study of the medical records of admissions due to CES at IOT in the period 2005–2015 with diagnosis of CES and neuropathic bladder. The following variables were analyzed: gender, age, etiology of the disease, topographic level of the injury, time interval between injury and diagnosis, presence of neurogenic bladder, time interval between diagnosis of the CES and surgery, and reversal of the deficit or of the neurogenic bladder.
Results
Since this is a rare disease, with a low global incidence, it was not possible, just with the current study to establish statistically significant correlations between the variables and outcomes of the disease. However, this study demonstrates the shortcomings of the Brazilian public health system, both with the initial management of these patients and the need for urgent surgical treatment.
Conclusion
The study shows that despite well-defined basis for the conduct of CES, a higher number of sequelae caused by the pathology is observed in Brazil. The delay in diagnosis and, therefore, for definitive treatment, remains as the major cause for the high number of sequelae. Level of evidence: 4, case series.
Keywords: Cauda equina, Intervertebral disc displacement, Neurogenic urinary bladder
Resumo
Objetivo
Analisar as características e os desfechos dos casos internados por síndrome da cauda equina (SCE) no Instituto de Ortopedia e Traumatologia (IOT) da Faculdade de Medicina da Universidade de São Paulo de 2005-2015. Secundariamente, este artigo é a continuação do trabalho epidemiológico de mesma base publicado em 2013 e servirá de base para outros estudos comparativos com vistas a um entendimento maior da doença e de sua epidemiologia.
Métodos
Estudo retrospectivo dos prontuários das internações por SCE no IOT de 2005 a 2015 com diagnósticos de SCE e bexiga neuropática. As seguintes variáveis foram analisadas: sexo, idade, etiologia da doença, nível topográfico da lesão, tempo de história da lesão até o diagnóstico, presença de bexiga neurogênica, tempo entre o diagnóstico da SCE e a cirurgia e reversão do déficit ou da bexiga neurogênica.
Resultados
Por se tratar de uma doença rara, com uma incidência global baixa, não foi possível, somente com o estudo atual, estabelecer correlações estatisticamente significativas entre as variáveis analisadas e os desfechos da doença. Porém, este estudo continua a evidenciar as deficiências do sistema público de saúde brasileiro, tanto no manejo inicial desses pacientes quanto na necessidade de tratamento cirúrgico de urgência.
Conclusão
O trabalho mostra que, apesar de bem definidas as bases para conduta da SCE, observa-se no Brasil um número maior de sequelas causadas pela patologia. O atraso no diagnóstico e, a partir desse, no tratamento definitivo mantém-se como a causa para o alto número de sequelas. Nível de evidência: 4, série de casos.
Palavras-chave: Cauda equina, Deslocamento do disco intervertebral, Bexiga urinária neurogênica
Introduction
Cauda equina syndrome (CSE) is classically characterized by the compression of the distal lumbar, sacral, and coccygeal nerve roots at the end of the conus medullaris at the L1 and L2 vertebral level.1 Although this disease has a low incidence in the population,2 ranging from 1:33,000 to 1:100,000 inhabitants,3 its sequelae still generate high public healthcare costs.
The clinical signs characteristic of the pathology are: severe back pain, often accompanied by sciatica; saddle anesthesia4, 5; sphincter and sexual dysfunction; and lower limb weakness.6, 7, 8 The presence of all these signs simultaneously is not required for diagnosis.6 The clinical history and the neurological examination lead to the need for diagnostic confirmation through complementary exams such as computed tomography (CT) and the gold standard, magnetic resonance imaging (MRI).1 MRI is mandatory for determining compression topography and etiology.8
Among the causes of compression, the following are noteworthy: extruded disc herniation5, 9 (Fig. 1, Fig. 2), tumor lesions10 (Fig. 3), vertebral fractures,11, 12, 13 canal stenoses,14 infections,13 surgical manipulation,15, 16 spinal anesthesia,17 ankylosing spondylitis,18, 19 and gunfire wounds.20 Some reports also indicate its onset after chiropractic manipulation.21 This is an orthopedic emergency and its treatment of choice continues to be surgical decompression,13, 22, 23, 24, 25 which, if performed as early as possible,25, 26, 27, 28 reduces neurological damage4, 29, 30 and improves the prognosis.26, 27, 31
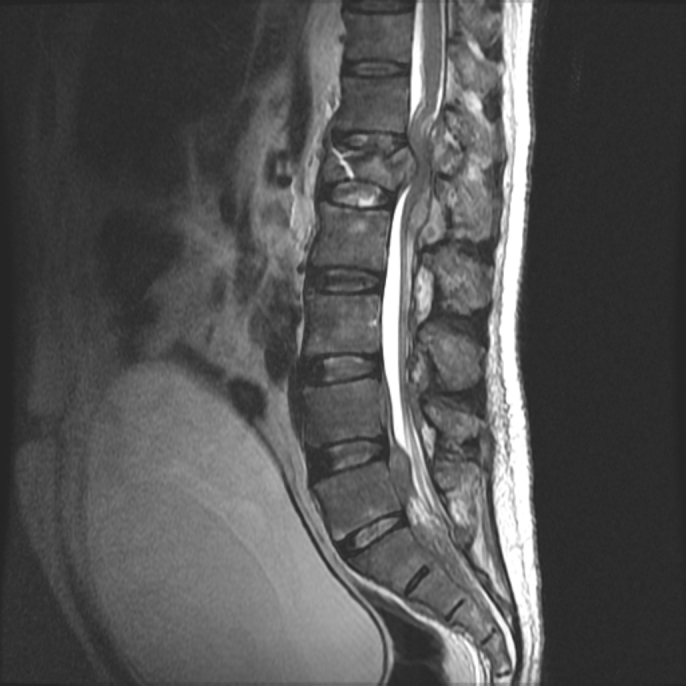
Fig. 1.

Magnetic resonance imaging (T1) showing a protruding disc herniation L5–S1 in a 37-year-old female patient admitted to hospital due to cauda equina syndrome.
Fig. 2.

Magnetic resonance imaging (T1) shows an extruded disc herniation in L4–L5 in a 49-year-old female patient.
Fig. 3.
Pathologic L1 fracture in a 55-year-old male patient admitted to hospital with a history of low back pain that started three months earlier, and one week of neurological deficit and sphincter loss of control.
The primary objective of this study was to analyze, through cross reference data, the characteristics of the cases and outcome of patients admitted to hospital due to CES at the IOT-HC-FMUSP Spine Group. Secondarily, it will continue to serve as a basis for other comparative studies, aiming to achieve a greater understanding of the disease and its epidemiology.
Methods
This was a retrospective study of the medical records of patients admitted to hospital due to CES at the IOT from 2005 to 2015. All records with diagnoses classified by the International Classification of Diseases (ICD) with codes G83.4 and N31.0/N31.1/N31.2 (CES and neuropathic bladder, respectively) were investigated.
From these records, all those who presented spinal cord injuries above the level of the T12 vertebra were excluded. Patients with confirmed CES diagnosis, detailed clinical history and neurological examination at admission, and CT and MRI assessment of the lumbosacral spine were included. The medical records of all cases included in this sample featured a well-documented report of the initial and postoperative physical examinations and of disease progress.
The following variables were analyzed in the sample: gender, age, disease etiology, topographic level of the lesion, time from injury to diagnosis, level of neurological deficit (considered as being the last normal topographic level regarding strength and sensitivity), presence of neurogenic bladder, time between CES diagnosis and surgical procedure, and reversal of the deficit or of the neurogenic bladder.
At this medical facility, the clinical care, the imaging tests (MRI and CT), and the treatment of this pathology (emergency decompression) are very well established and standardized. Outcomes (variables) were analyzed by the descriptions of case history and initial neurological physical examination (admission to the emergency room), of the first postoperative day, and of outpatient follow-up visits at two weeks, and 90–120 days after hospital discharge.
The data were submitted to statistical analysis.
Results
As shown in Table 1, most of the 22 patients included in this study were referred to this medical service more than 48 h after symptom onset.
Table 1.
Time from symptom onset to diagnosis.
| Time | Number of patients (n = 22) | % |
|---|---|---|
| Over 48 h | 17 | 77 |
| Less than 48 h | 5 | 23 |
Table 2 presents the most prevalent etiologies, in descending order, and their respective percentages.
Table 2.
Etiologies.
| Etiology | Number of patients (n = 22) | % |
|---|---|---|
| Herniation | 16 | 72.7 |
| Tumor | 3 | 13.6 |
| Trauma | 2 | 9.1 |
| Vascular | 1 | 4.5 |
The gender distribution was nine male patients (41%) and 13 female patients (59%). The patients had a mean age of 44.16 ± 12.83 years, ranging from 22 to 64 years.
The list of the topographic levels affected are shown in Table 3.
Table 3.
Injury level.
| Injury level | Number of patients (n = 22) | % |
|---|---|---|
| T12 | 1 | 4.5 |
| T12-L1 | 1 | 4.5 |
| L1 | 1 | 4.5 |
| L2–L3 | 1 | 4.5 |
| L3–L4 | 2 | 9.1 |
| L4–L5 | 9 | 41 |
| L5–S1 | 7 | 31.8 |
Table 4 presents the relationships between the time of onset of symptoms, diagnosis, and surgery.
Table 4.
Time of symptom onset × diagnosis × surgery.
| Median time | Range | |
|---|---|---|
| Time between CES symptom onset and diagnosis | 11 ± 24 days | 2–90 days |
| Time between diagnosis and surgery | 4 ± 6 days | 1–25 days |
| Time between symptom onset and surgery | 18 ± 24 days | 5–115 days |
After decompression surgery, the evolution of the deficit and of the neurogenic bladder were assessed on the first postoperative day, at two weeks outpatient follow-up visit, and at an outpatient follow-up visit up to 120 days. In these assessments, improvement was considered as any neurological recovery in relation to the initial deficit and the complete resolution of the neurogenic bladder. Table 5 describes the results.
Table 5.
Postoperative evolution.
| After decompression and up to 120 postoperative days | Number of patients (n = 22) | % |
|---|---|---|
| Permanence of initial neurological deficit | 8 | 36 |
| Permanence of neurogenic bladder | 14 | 64 |
Discussion
CES is still an often-neglected disease in emergency services, causing significant social and financial costs. In the present study, 77% of the patients (n = 17) sought or were referred to this medical facility much later than the recommended 48 h (Fig. 3).
Its pathogenesis remains under investigation.32 The two main hypotheses revolve around mechanical compression or ischemia to the cauda equina.33 The data found in this study show that the main etiology found was disc herniation (72.7%), followed by tumor (13.6%),6, 10 trauma (9.1%),3 and vascular problems (4.5%).1 In reality, these etiologies in some way combine compressive and/or ischemic mechanisms.
In line with the finding of disc pathology as the most prevalent etiology, the mean age range of 44,16 ± 12.83 years of the present sample is that with the highest occurrence of disc herniation34; the highest prevalence of topographic and neurological levels was at L4–L5/L5–S1 (72.7%).34
In the present study, among the cases of CES caused by herniated discs, a difference between the percentage of male (41%)12 and female patients (59%)17 was observed, albeit not statistically significant, which is in agreement with the gender distribution of this etiology in the literature.6, 31, 34
In the present study, a long delay between symptom onset and the definitive diagnosis of CES was observed (median time: 11 ± 24 days, range: 2–90 days). The authors believe that there is still a great confusion among healthcare professionals regarding the classic signs and symptoms of the disease, which hinders its rapid diagnosis. The public healthcare system still suffers from low availability of complementary diagnostic resources in primary healthcare services, which is another potential cause of delay. Another factor is the low socioeconomic level of some patients, which delays the search for medical help. The overcrowding of public health services and the long queues can also be mentioned as possible aggravating factors.
Urgent surgical decompression is still the most effective treatment,2, 8, 24, 35, 36 despite the fact that the exact time limit for surgery is debated by different authors.9, 31 It is the only safe way to prevent injury progression to the point of permanent deficits.8, 19, 35, 36
At this medical facility, patient care is based on a well-defined protocol, with ready access to complementary radiological investigation. Nevertheless, the patients in the present sample did not undergo satisfactory emergency surgical decompression (median time between diagnosis and surgery: 4 ± 6 days, range: 1–25 days). The main possible explanation for the delay in the surgical management of these cases is the great volume of procedures in our operating rooms, that include orthopedic specialties other than spinal surgery.
Regarding neurological sequelae, that include permanent motor and sensory deficits and neurogenic bladder, persistence of the initial deficit was observed in 36%11 and of neurogenic bladder in 64%18 of patients submitted to a decompression procedure. Due to the limited number of cases, statistically significant correlations between the variables were not observed, but there was a tendency toward better prognosis in the patients operated close to the recommended optimal time.
Conclusion
The study demonstrates that, although the basis for CES conduct is well defined, a greater prevalence of sequelae caused by the pathology is observed in Brazil. The delay in diagnosis and in definitive treatment remains the cause for the high number of sequelae. Level of evidence: 4, series of cases.
Conflicts of interest
The authors declare no conflicts of interest.
Footnotes
Study conducted at the Laboratório de Investigação Médica do Sistema Músculo-Esquelético (LIM 41), Departamento de Ortopedia e Traumatologia, Faculdade de Medicina, Universidade de Sao Paulo (FMUSP), São Paulo, SP, Brazil.
References
- 1.Curtin P., Sankar R., Fogarty E.E. It's never too late: cauda equine syndrome in an octogenarian. Injury Extra. 2005;36:242–244. [Google Scholar]
- 2.Germon T., Ahuja S., Casey A.T., Todd N.V., Rai A. British Association of Spine Surgeons standards of care for cauda equina syndrome. Spine J. 2015;15(3 Suppl.):S2–S4. doi: 10.1016/j.spinee.2015.01.006. [DOI] [PubMed] [Google Scholar]
- 3.Anthony S. Cauda equina syndrome. Med Protect Soc Casebook. 2000;20:9–13. [Google Scholar]
- 4.Markham D.E. Cauda equine syndrome: diagnosis, delay, and litigation risk. Curr Orthop. 2004;18(1):58–62. [Google Scholar]
- 5.Gardner A., Gardner E., Morley T. Cauda equina syndrome: a review of the current clinical and medico-legal position. Eur Spine J. 2011;20(5):690–697. doi: 10.1007/s00586-010-1668-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Kostuik J.P., Harrington I., Alexander D., Rand W., Evans D. Cauda equina syndrome and lumbar disc herniation. J Bone Joint Surg Am. 1986;68(3):386–391. [PubMed] [Google Scholar]
- 7.Kennedy J.G., Soffe K.E., McGrath A., Stephens M.M., Walsh M.G., McManus F. Predictors of outcome in cauda equina syndrome. Eur Spine J. 1999;8(4):317–322. doi: 10.1007/s005860050180. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Fairbank J., Mallen C. Cauda equina syndrome: implications for primary care. Br J Gen Pract. 2014;64(619):67–68. doi: 10.3399/bjgp14X676988. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Ahn U.M., Ahn N.U., Buchowski J.M., Garrett E.S., Sieber A.N., Kostuik J.P. Cauda equina syndrome secondary to lumbar disc herniation: a meta-analysis of surgical outcomes. Spine (Phila Pa 1976) 2000;25(12):1515–1522. doi: 10.1097/00007632-200006150-00010. [DOI] [PubMed] [Google Scholar]
- 10.Kebaish K.M., Awad J.N. Spinal epidural hematoma causing acute cauda equine syndrome. Neurosurg Focus. 2004;16(6):e1. [PubMed] [Google Scholar]
- 11.Harrop J.S., Hunt G.E., Jr., Vaccaro A.R. Conus medullaris and cauda equina syndrome as a result of traumatic injuries: management principles. Neurosurg Focus. 2004;16(6):e4. doi: 10.3171/foc.2004.16.6.4. [DOI] [PubMed] [Google Scholar]
- 12.Thongtrangan I., Le H., Park J., Kim D.H. Cauda equina syndrome in patients with low lumbar fractures. Neurosurg Focus. 2004;16(6):e6. [PubMed] [Google Scholar]
- 13.Kostuik J.P. Medicolegal consequences of cauda equina syndrome: an overview. Neurosurg Focus. 2004;16(6):e8. doi: 10.3171/foc.2004.16.6.7. [DOI] [PubMed] [Google Scholar]
- 14.Cohen D.B. Infectious origins of cauda equina syndrome. Neurosurg Focus. 2004;16(6):e2. doi: 10.3171/foc.2004.16.6.2. [DOI] [PubMed] [Google Scholar]
- 15.Jensen R.L. Cauda equina syndrome as a postoperative complication of lumbar spine surgery. Neurosurg Focus. 2004;16(6):e7. doi: 10.3171/foc.2004.16.6.6. [DOI] [PubMed] [Google Scholar]
- 16.Morandi X., Riffaud L., Houedakor J., Amlashi S.F., Brassier G., Gallien P. Caudal spinal cord ischemia after lumbar vertebral manipulation. Joint Bone Spine. 2004;71(4):334–337. doi: 10.1016/S1297-319X(03)00154-4. [DOI] [PubMed] [Google Scholar]
- 17.Ozgen S., Baykan N., Dogan I.V., Konya D., Pamir M.N. Cauda equina syndrome after induction of spinal anesthesia. Neurosurg Focus. 2004;16(6):e5. doi: 10.3171/foc.2004.16.6.5. [DOI] [PubMed] [Google Scholar]
- 18.Rubenstein D.J., Alvarez O., Ghelman B., Marchisello P. Cauda equina syndrome complicating ankylosing spondylitis: MR features. J Comput Assist Tomogr. 1989;13(3):511–513. doi: 10.1097/00004728-198905000-00029. [DOI] [PubMed] [Google Scholar]
- 19.Bartleson J.D., Miller G.M., Lanzino G. Cauda equina syndrome associated with longstanding instrumented spinal fusion. World Neurosurg. 2013;79(3–4) doi: 10.1016/j.wneu.2011.12.014. 594.e5–8. [DOI] [PubMed] [Google Scholar]
- 20.Flores L.P., Nascimento Filho J.S., Pereira Neto A., Suzuki K. Prognostic factors related to gunshot wounds to the spine in patients submitted to laminectomy. Arq Neuropsiquiatr. 1999;57(3B):836–842. doi: 10.1590/s0004-282x1999000500016. [DOI] [PubMed] [Google Scholar]
- 21.Solheim O., Jorgensen J.V., Nygaard O.P. Lumbar epidural hematoma after chiropractic manipulation for lower-back pain: case report. Neurosurgery. 2007;61(1):E170–E171. doi: 10.1227/01.neu.0000279740.61048.e2. [DOI] [PubMed] [Google Scholar]
- 22.Gleave J.R., Macfarlane R. Cauda equina syndrome: what is the relationship between timing of surgery and outcome? Br J Neurosurg. 2002;16(4):325–328. doi: 10.1080/0268869021000032887. [DOI] [PubMed] [Google Scholar]
- 23.O’Laoire S.A., Crockard H.A., Thomas D.G. Prognosis for sphincter recovery after operation for cauda equina compression owing to lumbar disc prolapse. Br Med J (Clin Res Ed) 1981;282(6279):1852–1854. doi: 10.1136/bmj.282.6279.1852. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Theys T., Kho K.H. The saddle and the horse's tail: cauda equina syndrome. JAMA Neurol. 2014;71(7):914–915. doi: 10.1001/jamaneurol.2013.6008. [DOI] [PubMed] [Google Scholar]
- 25.Sonntag V.K. Why not decompress early? The cauda equina syndrome. World Neurosurg. 2014;82(1–2):70–71. doi: 10.1016/j.wneu.2014.03.016. [DOI] [PubMed] [Google Scholar]
- 26.Chau A.M., Xu L.L., Pelzer N.R., Gragnaniello C. Timing of surgical intervention in cauda equina syndrome: a systematic critical review. World Neurosurg. 2014;81(3-4):640–650. doi: 10.1016/j.wneu.2013.11.007. [DOI] [PubMed] [Google Scholar]
- 27.Bydon M., Gokaslan Z.L. Time to treatment of cauda equina syndrome: a time to reevaluate our clinical decision. World Neurosurg. 2014;82(3–4):344–345. doi: 10.1016/j.wneu.2014.03.006. [DOI] [PubMed] [Google Scholar]
- 28.Nater A., Fehlings M.G. The timing of decompressive spinal surgery in cauda equina syndrome. World Neurosurg. 2015;83(1):19–22. doi: 10.1016/j.wneu.2014.03.017. [DOI] [PubMed] [Google Scholar]
- 29.Hussain S.A., Gullan R.W., Chitnavis B.P. Cauda equina syndrome: outcome and implications for management. Br J Neurosurg. 2003;17(2):164–167. doi: 10.1080/0268869031000109098. [DOI] [PubMed] [Google Scholar]
- 30.Shapiro S. Medical realities of cauda equina syndrome secondary to lumbar disc herniation. Spine (Phila Pa 1976) 2000;25(3):348–351. doi: 10.1097/00007632-200002010-00015. [DOI] [PubMed] [Google Scholar]
- 31.Chang H.S., Nakagawa H., Mizuno J. Lumbar herniated disc presenting with cauda equina syndrome. Long-term follow-up of four cases. Surg Neurol. 2000;53(2):100–104. doi: 10.1016/s0090-3019(99)00180-9. [DOI] [PubMed] [Google Scholar]
- 32.Shephard R.H. Diagnosis and prognosis of cauda equina syndrome produced by protrusion of lumbar disk. Br Med J. 1959;2(5164):1434–1439. doi: 10.1136/bmj.2.5164.1434. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Kohles S.S., Kohles D.A., Karp A.P., Erlich V.M., Polissar N.L. Time-dependent surgical outcomes following cauda equina syndrome diagnosis: comments on a meta-analysis. Spine (Phila Pa 1976) 2004;29(11):1281–1287. doi: 10.1097/00007632-200406010-00019. [DOI] [PubMed] [Google Scholar]
- 34.McCarthy M.J., Aylott C.E., Grevitt M.P., Hegarty J. Cauda equina syndrome: factors affecting long-term functional and sphincteric outcome. Spine (Phila Pa 1976) 2007;32(2):207–216. doi: 10.1097/01.brs.0000251750.20508.84. [DOI] [PubMed] [Google Scholar]
- 35.Qureshi A., Sell P. Cauda equina syndrome treated by surgical decompression: the influence of timing on surgical outcome. Eur Spine J. 2007;16(12):2143–2151. doi: 10.1007/s00586-007-0491-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Fuso F.A., Dias A.L., Letaif O.B., Cristante A.F., Marcon R.M., de Barros T.E. Epidemiological study of cauda equina syndrome. Acta Ortop Bras. 2013;21(3):159–162. doi: 10.1590/S1413-78522013000300006. [DOI] [PMC free article] [PubMed] [Google Scholar]