
Figure 1. HRs and 95% CIs for total and CVD mortality, sensitivity analyses.
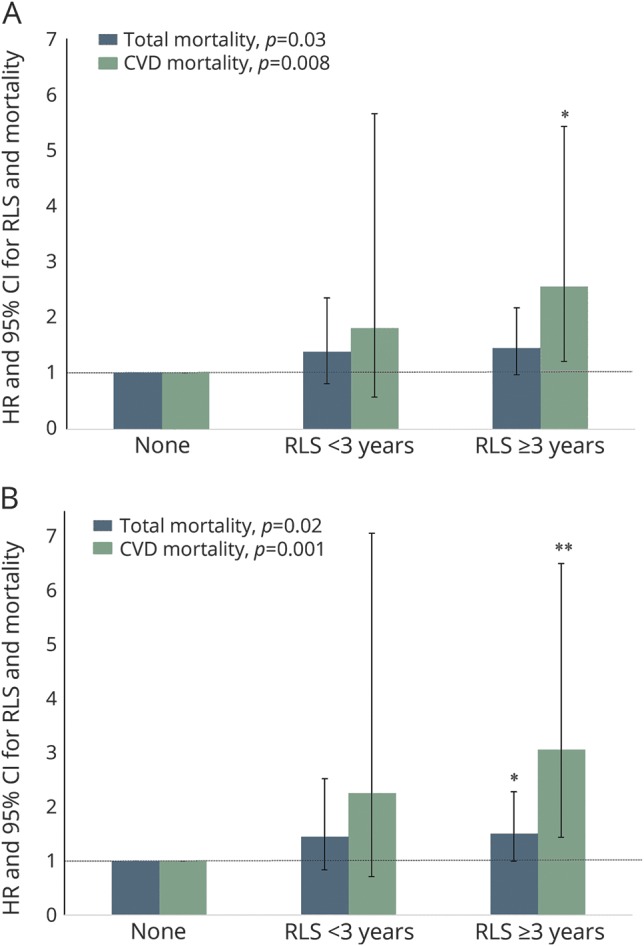
HRs and CIs are according to RLS duration among 21,063 participants (A) without snoring, short (≤6 h/d) or prolonged (≥9 h/d) sleep duration, arthritis, diabetes mellitus, Parkinson disease, obesity, and use of antidepressants or iron-specific supplements or (B) further excluding death in the first 2 years of follow-up. The models were adjusted for age (months), race (white, yes/no), smoking status (never smoker, former smoker, or current smoker), alcohol consumption (0, 0.1–4.9, 5.0–9.9, 10.0–14.9, and ≥15 g/d), physical activity (quintiles), Adjusted Healthy Eating Index (quintiles), history of hypertension and hypercholesterolemia, use of estrogen hormone therapy (premenopausal, postmenopausal with no use, past user, or current user), and regular use of aspirin (yes/no). Linear trends were tested for significance by treating the year of RLS diagnosis as a continuous variable. CI = confidence interval; CVD = cardiovascular disease; HR = hazard ratio; RLS = restless legs syndrome. *p < 0.05 relative to women without RLS; **p < 0.01 relative to women without RLS.