

Abstract
Substance abuse and its consequences are major health hazards in the world. Opium addiction is a common form of substance abuse in Iran. Adulteration of illegal substances in the process of production and distribution of the drug in black market with many types of materials have been reported. One of the main goals of the adulteration of illegal substances is cutting of the substance for deal and increase of the weight for more benefit. However, adding of adulterating agents to illegal drugs could be considered as a cause of nonspecific and rare toxicity during substance abuse. Although the presence of lead in street-level heroin, marijuana, and amphetamines has been reported from some countries previously, recently, several reports suggested lead poisoning in Iranian opium addicts. Adulteration of opium with lead is a new source of lead poisoning in Iran in which the opium abuse is frequent and it could be a new health problem in the future. In this regard, evaluation of blood lead level would be important for early diagnosis of lead poisoning in opium addicts.
Keywords: Iran, lead, opioid-related disorders, opium, poisoning
Introduction
Lead is a bluish-gray metal and highly toxic element. Its properties such as corrosion resistance, density, and low melting point make it a familiar metal with high applications in the industry.[1,2] It can induce acute and chronic poisoning in human.[1] Lead is considered as a toxic substance affecting multiple organ systems.[3] Its poisoning can be due to occupational or environmental exposures, for example, car exhausts, contaminated food, industrial emission, and contaminated soil.[4] Ingestion, inhalation, or dermal exposure to the lead contamination sources can cause notable poisoning.[4]
Clinical presentations of lead toxicity are nonspecific including abdominal pain, anorexia, constipation, myalgia, decreased libido, irritability, seizure, and anemia.[3] Abdominal pain in lead poisoning can be misdiagnosed as an acute abdomen.[5]
Nowadays, the incidence of acute lead poisoning has declined, but the chronic lead poisoning still exists in various parts of the world.[2] The majority of elevated blood lead levels (BLLs) in adults come from occupational and industrial exposures.[6,7] Lead exposure is usually considered when a patient's history is remarkable to well-known sources of lead such as in occupational and industrial settings. However, unusual causes of lead intoxication have been described. One of the uncommon sources of lead poisoning is lead-adulterated illegal substances abuse such as marijuana and methamphetamine.[8,9,10]
Substance abuse is a major problem of public health in Iran.[11,12] Opium and its derivatives is the most common drug that is abused in Iran.[11] Recently, few reports about lead poisoning in opium abusers in Iran have been reported.[13,14,15,16,17,18] In addition, researchers reported the presence of lead in opium in the southeast of Iran.[19] It seems that the lead is present as impurities and adulterants in illicit opium, which smuggled and distributed in Iran. In this article, we reviewed the reports of lead poisoning in opium abusers in Iran.
Methods
A literature search of online databases (PubMed, Web of Science, Google Scholar, and Scopus) for studies investigated lead poisoning in opium abusers in Iran was performed.
Search criteria
The search terms were “opium/opium abuse,” and “lead poisoning/toxicity” or “lead-contaminated opium.” The data were collected from March 2000 to November 2016. There were no language restrictions. All types of papers were included. We also reviewed the reference lists of identified publications and abstract book of national congresses for additional studies. The title and abstract of each article were reviewed to make a decision for eligibility of the paper. Full text of all eligible papers was obtained. Finally, 18 articles have been included in this review.
Results
Lead poisoning in opium abusers
Beigmohammadi et al. reported a 40-year-old male with opium addiction history with a headache, nausea and abdominal pain, and weakness in his lower and upper extremities without a definitive diagnosis who was admitted in Intensive Care Unit (ICU). He did not have an occupational lead history in his past medical history. He had anemia, slightly elevated liver function tests, total bilirubin, and erythrocyte sedimentation rate. Electromyography and nerve conduction velocity results and neurologic examination were abnormal. His BLL was more than 200 μg/dL. He was treated with British Anti-Lewisite (BAL) and calcium disodium edetate CaNa2 EDTA. Following ICU discharge, he was quadriplegic although BLL was decreased and all paraclinical findings were normal.[15]
Hayatbakhsh Abbasi et al. conducted a cross-sectional study to compare the serum lead levels between opium addicts (n = 50) and nonaddicts (n = 43). They were matched with sex and age. The serum level of lead in opium addicts was higher than nonaddicts.[16]
In another study which has been conducted by Salehi et al., they analyzed the BLL in opium addicts (n = 22) who used oral opium and control group (n = 22) which was matched with for age and sex. The BLL in opium addicts had a range of 7.2–69.9 μg/dL (mean of 21.9 ± 13.2 μg/dL). In control group, BLL was 4.1–17.4 μg/dL (mean of 8.6 ± 3.5 μg/dL). The result was statistically significant (P < 0.0001). In the patient group, BLL had a significant correlation with the amount of ingested opium (r = 0.65, P < 0.01). However, there was no significant correlation with duration of opium ingestion in the patient group. They concluded that screening of BLL should be considered in the treatment of opium addicts.[20]
Masoodi et al. (2006) showed that lead poisoning in three patients presented with diffuse abdominal pain, anemia, constipation, nausea, vomiting, and abnormal liver function tests. A history of oral consumption of opium was presented in all of the patients, and none of them reported known occupational lead exposure. Lead poisoning was confirmed by analysis of BLL. Ingestion of lead-contaminated opium was the cause of poisoning.[13]
Salman-Roghani and Foroozan reported a 46-year-old opium-addicted man with hepatobiliary tract problems. He complained of abdominal pain, constipation, weakness, and neurologic abnormalities (tremor and proximal weakness). BLL was 90 μg/dL, and the patient was treated with the diagnosis of lead toxicity.[21]
Verheij et al. described a case of the 40-year-old Iranian man anemia and abnormality in liver function tests with severe abdominal pain, In his past medical history, he was suffering from multiple sclerosis. The patient used opium as a painkiller, regularly. Basophilic stippling of erythrocytes proposed lead poisoning. In this patient, the probable source of poisoning was adulterated opium. BLL were strongly elevated (86 μg/dL). The authors showed lead-induced hepatotoxicity in the case. In the liver biopsy, pathologic findings of hepatotoxicity such as active hepatitis lymphocytic cholangitis, with steatosis, cholestasis and hemosiderosis have been reported in the patient. After chelating therapy, liver enzymes returned to normal, suggesting reversibility of the histological findings.[22]
Soltaninejad et al. in a descriptive and retrospective study presented 25 cases of lead poisoning who were admitted to a referral poison center in Tehran between the years 2002 and 2007. In seven patients, opium addiction was the only source of lead poisoning. None of them had a well-known occupational exposure to lead. The average age of the patients was 38.7 ± 9.3 years and the average BLL was 109 ± 37.6 μg/dL. Inhalation was the route of opium abuse in 4 patients. Others abused opium orally.[23]
Froutan et al. reported opium addicts with abdominal pain who were presented to the gastrointestinal center of a referral hospital in Tehran during 2008. Patients who had occupational exposure to lead were excluded from the study. During this period, 42 patients (all male) with an average age of 46.9 ± 10.1 years were included in the study. Average BLL was 51.17 ± 27.96 μg/dl. A total of 22 patients (52.6%) had lead poisoning. A significant relation was found between lead poisoning and mode of opium abuse. The relation between lead poisoning and duration of opium addiction was not observed. However, a statistically significant relation was found between lead intoxication and abnormal liver function tests, urine tests, electrocardiogram, presence of basophilic stippling, and hyperuricemia.[5]
Meybodi et al. demonstrated that of the 240 patients diagnosed with lead poisoning, 25 patients admitted to opium use. There were 24 (96%) men and one (4%) woman. The average age of the patients was 41.8 ± 13.5 years. The duration of addiction to oral opium differed widely (range 3 months to 40 years). BLL were 145 ± 61 (range: 61–323) μg/dL. There was no significant statistical correlation between the duration of addiction and BLL in addicted patients (r = −0.142, P = 0.54). The most common complaints were anorexia (96%), abdominal pain (92%), weight loss >10% within a 2-month period (84%), constipation (88%), and nausea (56%). The most common musculoskeletal complaint was muscle weakness (92%). Other complaints included wrist drop (4%), pain in the extremities (88%), paresthesia (56%), and reduced vision (20%) and hearing (8%). Three (12%) patients initially presented with acute abdomen (bowel obstruction and peritonitis).[24]
Amiri and Amini evaluated the BLL of 39 Iranian opium addicts and made a comparison with healthy individuals as a control group in a hospital in Tehran. All the cases were male. The addicts were used opium orally or by inhalation. The mean age was 48.6 ± 7.3 years. The control group (39 individuals) was matched with the addicts with regard to age and sex and with a mean age of 44.8 ± 5.6 years. The mean BLL was found to be significantly lower (P = 0.0001) in control group (16.70 ± 12.51 μg/dL) compared to addicts (57.04 ± 46.03 μg/dL). There was a significant difference (P = 0.0451) in BLL according to age. Furthermore, a tendency (P = 0.048) toward increasing BLL with respect to body mass index (BMI) was observed due to opium abuse, but there was no significant variation between BLL and BMI when the control group was considered (P = 0.35).[25]
Mokhtarifar et al. reported a 55-year-old man presented to the emergency department with abdominal pain, icterus, high serum alkaline phosphatase levels, and normocytic anemia. He had opium abuse history for 20 years. Clinical and paraclinical findings including the Burton's sign and generalized ileus on abdominal X-ray have been observed. BLL was 150 μg/dL. Investigation of the patient's history failed to reveal any exposure to lead. Magnetic resonance imaging and abdominal ultrasonography were performed for rule out the other reasons of cholestasis. Liver biopsy showed focal canalicular cholestasis and mild portal inflammation. The patient had severe nausea, vomiting, and a single generalized tonic–colonic seizure 4 days after admission. Neurologic evaluations including brain computed tomography scan, and magnetic resonance imaging, and magnetic resonance venography were normal. The patient was treated with CaNa2 EDTA and BAL for five days. The patient's liver biochemical tests abnormality recovered. Gastrointestinal presentations subsided, and the patient was discharged with good condition.[26]
Domeneh et al. in a cross-sectional study among 86 opium addicts who were referred to five detoxification centers in Tehran, reported that BLL was higher in oral opium-dependent group (11.75 ± 6.06 μg/dL) than inhalation opium addict (7.07 ± 3.61 μg/dL) and healthy (6.05 ± 1.83 μg/dL) groups.[27]
Khatibi-Moghadam et al. reported that the mean value BLL in 40 opium addicts was 7.14 ± 1.41 μg/dL compared to 5.42 ± 1.46 μg/dL in healthy control group. The mean value of urine lead level was 2.62 ± 0.83 μg/dL and 2.50 ± 0.76 μg/dL in patient and control groups, respectively. They showed a significant correlation between BLL with duration of opium addiction.[28]
Azizi et al. reported a lead-intoxicated case in a 46-year-old Iranian man who resident in the UK with opium addiction history. He had a 4-day history of colicky abdominal pain and constipation and several weeks of irritability and malaise. He had smoked 10 g of opium per week for a year and a half. On examination, he had abdominal pain, nausea, vomiting, diffuse abdominal tenderness, and fecal loading. Furthermore, hemolytic anemia and basophilic stippling have been shown in hematologic tests. The patient's serum lead concentration was substantially elevated. After chelation therapy, he has recovered clinically and biochemically.[29]
Lead poisoning due to abuse of lead-contaminated opium
Soltaninejad et al. reported a fatal lead poisoning in a 27-year-old man with 2 years of opium addiction history. Lead poisoning was confirmed by analysis of BLL (150 μg/dL) and clinical and postmortem autopsy findings. Lead content has been determined in opium sample which ingested by the decedent by atomic absorption spectrophotometer as 5.6%w/w.[30,31]
Fatemi et al. reported a lead poisoning in a 25-year-old man with 6-year history of addiction to oral and inhalation opium. He presented with gastrointestinal presentations such as abdominal pain, nausea and vomiting, severe weight loss, generalized bone pain, and jaundice without hepatosplenomegaly and lymphadenopathy. Pallor and jaundice were observed in his mucosa and bluish pigmentation was evident at the gum-teeth line. Liver enzymes and indirect bilirubin increased. Hemolytic anemia without autoimmune origin and erythroid hyperplasia has been shown in bone marrow biopsy. The serum lead level was 350 μg/dL. Furthermore, the lead was detected in opium sample that the patient used. The patient was treated with standard CaNa2 EDTA, and BAL and symptoms were eliminated during 2 weeks after chelating therapy.[14]
Aghaee-Afshar et al. analyzed the lead content in ten opium samples which were selected randomly from the opium seized by Police Department in Kerman province (South-east of Iran) by atomic absorption spectrophotometer. The mean concentration of lead in the samples ± standard error of mean was 1.88 ± 0.35 ppm. The minimum and maximum lead concentrations in the samples were 0.7308 ppm and 3.5255 ppm, respectively.[19]
Jalili and Azizkhani reported a lead poisoning case in a 32-year-old man with opium addiction who presented to the emergency department with lower abdominal pain and constipation. In physical examination, he had mild abdominal tenderness and gingival discoloration. Laboratory findings showed a mild hypochromic, microcytic anemia with basophilic stippling of the erythrocytes. The BLL was 50 μg/dL and diagnosis of lead toxicity was made and the patient was treated with 2,3-dimercaptosuccinic acid. His signs and symptoms subsided over the next week and he was discharged. Analysis of the used opium sample showed 35.2 mg of lead per 100 g of opium.[17]
Moharari et al. reported two cases (Iranian father and son), with severe lead poisoning due to opium addiction. The patients have been hospitalized with regard to neurological symptoms (unconsciousness, delirium, and hyperirritability), gastrointestinal (icter, abdominal pain) and anemia. The older patient (68-year-old man) showed the neuropathy and electro encephalography symptoms including paralysis and absent deep tendon reflexes and low level of consciousness. The patients’ BLL indicated a high level of lead in both of them (≥150 μg/dL). Furthermore, the used sample of opium was sent to the laboratory, and analysis of lead in the sample showed a higher lead content. One of the patients died due to cardiovascular collapse.[32]
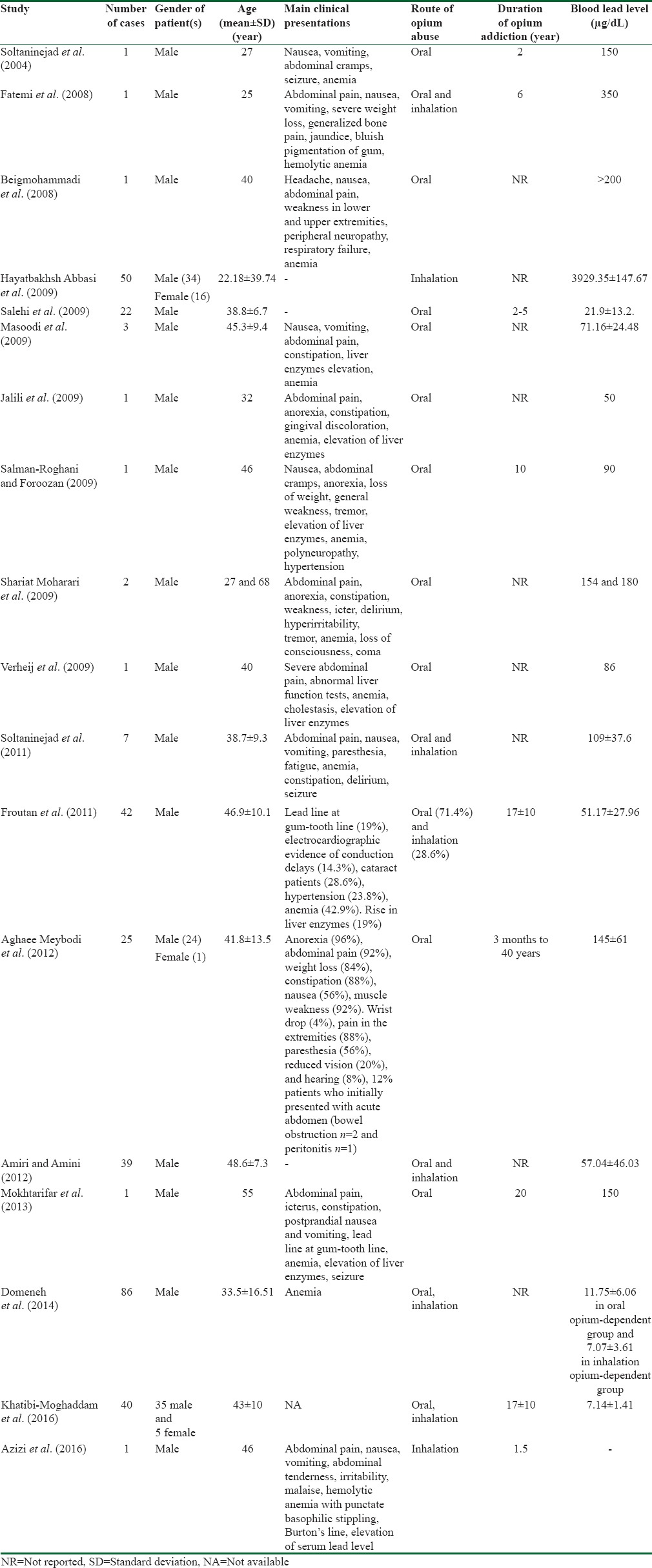
Table 1 summarizes clinical studies relevant to lead poisoning due to opium addiction in Iran.
Table 1.
Clinical studies relevant to lead poisoning due to opium addiction in Iran
Discussion
Although lead poisoning in industrial and occupational settings has decreased, the new forms of nonoccupational lead poisoning have increased. The presence of heavy and toxic metals such as arsenic in opium,[33,34,35,36] lead, and thallium in heroin samples as impurities and adulteration has been reported from some countries.[37,38,39,40,41] There are a few reports about lead poisoning due to abuse of lead-contaminated opioid worldwide, and in recent years, lead poisoning in opium addicts have been reported from Iran.
In this article, we reviewed 20 documents; from which, 18 studies reported 324 cases of lead poisoning in opium abusers in Iran during 2004–2016. According to these researches and medical evidences, it could be concluded that illegal opium samples in Iran have been contaminated with lead. It may be due to adulteration of opium by dealers, salesmen, and smugglers during the opium preparation and distribution in the black market to increase the weight of opium for more profit. The studies showed that there is a statistically significant correlation between BLL and route of opium abuse. Higher BLL was observed in patients with oral opium abuse. Furthermore, there is a significant correlation between BLL and amount of opium abuse. There are controversies with regard to the correlation between BLL and duration of opium abuse.
From this view, as a new health problem, lead poisoning should be considered in illegal opium abusers, mainly oral consumption, in Iran and other countries in which the opium abuse is frequent. As clinical manifestations of lead poisoning are nonspecific and may be misdiagnosed with other pathophysiological conditions, public health experts should be notified and conduct an assessment of the risk of lead poisoning in opium addicts.
Conclusions
Screening of BLL would be helpful for early diagnosis and treatment of lead poisoning in opium abusers to prevent complications of chronic lead poisoning.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Azizi MH, Azizi F. Lead poisoning in the world and Iran. Int J Occup Environ Med. 2010;1:81–7. [PubMed] [Google Scholar]
- 2.Pourmand A, Khedir Al-Tiae T, Mazer-Amirshahi M. Perspective on lead toxicity, a comparison between the United States and Iran. Daru. 2012;20:70. doi: 10.1186/2008-2231-20-70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Henretig FM. Lead. Gold Frank's Toxicologic Emergencies. In: Nelson LS, editor. 9th ed. New York: McGraw Hill; 2011. pp. 1266–80. [Google Scholar]
- 4.Homan CS, Brogan GX, Orava RS. Lead toxicity. Emergency Toxicology. In: Viccellio P, editor. 2nd ed. Philadelphia, PA: Lippincott-Raven; 1998. pp. 363–79. [Google Scholar]
- 5.Froutan H, Kashefi Zadeh A, Kalani M, Andrabi Y. Lead toxicity: A probable cause of abdominal pain in drug abusers. Med J Islam Repub Iran. 2011;25:16–20. [Google Scholar]
- 6.Pirkle JL, Brody DJ, Gunter EW, Kramer RA, Paschal DC, Flegal KM, et al. The decline in blood lead levels in the United States. The National Health and Nutrition Examination Surveys (NHANES) JAMA. 1994;272:284–91. [PubMed] [Google Scholar]
- 7.Tandon SK, Chatterjee M, Bhargava A, Shukla V, Bihari V. Lead poisoning in Indian silver refiners. Sci Total Environ. 2001;281:177–82. doi: 10.1016/s0048-9697(01)00845-2. [DOI] [PubMed] [Google Scholar]
- 8.Busse FP, Fiedler GM, Leichtle A, Hentschel H, Stumvoll M. Lead poisoning due to adulterated marijuana in Leipzig. Dtsch Arztebl Int. 2008;105:757–62. doi: 10.3238/arztebl.2008.0757. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Busse F, Omidi L, Timper K, Leichtle A, Windgassen M, Kluge E, et al. Lead poisoning due to adulterated marijuana. N Engl J Med. 2008;358:1641–2. doi: 10.1056/NEJMc0707784. [DOI] [PubMed] [Google Scholar]
- 10.Norton RL, Burton BT, McGirr J. Blood lead of intravenous drug users. J Toxicol Clin Toxicol. 1996;34:425–30. doi: 10.3109/15563659609013813. [DOI] [PubMed] [Google Scholar]
- 11.Mokri A. Brief overview of the status of drug abuse in Iran. Arch Iran Med. 2002;5:184–90. [Google Scholar]
- 12.Eskandarieh S, Nikfarjam A, Tarjoman T, Nasehi A, Jafari F, Saberi-Zafarghandi MB, et al. Descriptive aspects of injection drug users in Iran's national harm reduction program by methadone maintenance treatment. Iran J Public Health. 2013;42:588–93. [PMC free article] [PubMed] [Google Scholar]
- 13.Masoodi M, Zali MR, Ehsani-Ardakani MJ, Mohammad-Alizadeh AH, Aiassofi K, Aghazadeh R, et al. Abdominal pain due to lead-contaminated opium: A new source of inorganic lead poisoning in Iran. Arch Iran Med. 2006;9 [PubMed] [Google Scholar]
- 14.Fatemi R, Jafarzadeh F, Moosavi S, Afshar Amin F. Acute lead poisoning in an opium user: A case report. Gastroenterol Hepatol From Bed Bench. 2008;1:139–42. [Google Scholar]
- 15.Beigmohammadi MT, Aghdashi M, Najafi A, Mojtahedzadeh M, Karvandian K. Quadriplegia due to lead-contaminated opium – Case report. Middle East J Anaesthesiol. 2008;19:1411–6. [PubMed] [Google Scholar]
- 16.Hayatbakhsh Abbasi MM, Ansari M, Shahesmaeili A, Qaraie A. Lead serum levels in opium-dependent individuals. Addict Health. 2009;1:106–9. [PMC free article] [PubMed] [Google Scholar]
- 17.Jalili M, Azizkhani R. Lead toxicity resulting from chronic ingestion of opium. West J Emerg Med. 2009;10:244–6. [PMC free article] [PubMed] [Google Scholar]
- 18.Afshari R, Emadzadeh A. Short communication: Case report on adulterated opium-induced severe lead toxicity. Drug Chem Toxicol. 2010;33:48–9. doi: 10.3109/01480540903127340. [DOI] [PubMed] [Google Scholar]
- 19.Aghaee-Afshar M, Khazaeli P, Behnam B, Rezazadehkermani M, Ashraf-Ganjooei N. Presence of lead in opium. Arch Iran Med. 2008;11:553–4. [PubMed] [Google Scholar]
- 20.Salehi H, Sayadi AR, Tashakori M, Yazdandoost R, Soltanpoor N, Sadeghi H, et al. Comparison of serum lead level in oral opium addicts with healthy control group. Arch Iran Med. 2009;12:555–8. [PubMed] [Google Scholar]
- 21.Salman-Roghani H, Foroozan A. Lead poisoning, report of an interesting case. Govaresh. 2009;14:39–45. [Google Scholar]
- 22.Verheij J, Voortman J, van Nieuwkerk CM, Jarbandhan SV, Mulder CJ, Bloemena E, et al. Hepatic morphopathologic findings of lead poisoning in a drug addict: A case report. J Gastrointestin Liver Dis. 2009;18:225–7. [PubMed] [Google Scholar]
- 23.Soltaninejad K, Flückiger A, Shadnia S. Opium addiction and lead poisoning. J Subst Use. 2011;16:208–12. [Google Scholar]
- 24.Meybodi FA, Eslick GD, Sasani S, Abdolhoseyni M, Sazegar S, Ebrahimi F, et al. Oral opium: An unusual cause of lead poisoning. Singapore Med J. 2012;53:395–7. [PubMed] [Google Scholar]
- 25.Amiri M, Amini R. A comparison of blood-lead level (BLL) in opium-dependant addicts with healthy control group using the graphite furnace/atomic absorption spectroscopy (GF-AAS) followed by chemometric analysis. Iran Red Crescent Med J. 2012;14:488–91. [PMC free article] [PubMed] [Google Scholar]
- 26.Mokhtarifar A, Mozaffari H, Afshari R, Goshayeshi L, Akavan Rezayat K, Ghaffarzadegan K, et al. Cholestasis and seizure due to lead toxicity: A case report. Hepat Mon. 2013;13:e12427. doi: 10.5812/hepatmon.12427. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Domeneh BH, Tavakoli N, Jafari N. Blood lead level in opium dependents and its association with anemia: A cross-sectional study from the capital of Iran. J Res Med Sci. 2014;19:939–43. [PMC free article] [PubMed] [Google Scholar]
- 28.Khatibi-Moghadam H, Khadem-Rezaiyan M, Afshari R. Comparison of serum and urine lead levels in opium addicts with healthy control group. Hum Exp Toxicol. 2016;35:861–5. doi: 10.1177/0960327115607947. [DOI] [PubMed] [Google Scholar]
- 29.Azizi A, Ferguson K, Dluzewski S, Hussain T, Klein M. Chronic lead poisoning in an Iranian opium smoker resident in London. BMJ Case Rep 2016. 2016 doi: 10.1136/bcr-2016-215965. pii: Bcr2016215965. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Soltaninejad K, Akhgari M, Faryadi M. Case Report: Death Due to Lead Poisoning from Contaminated Opium. Abstract Book of the 8th Iranian Congress of Toxicology, Tehran, Iran; 6.8 December. 2004;71 [Google Scholar]
- 31.Soltaninejad K, Faryadi M, Akhgari M. Determination of lead in opium by flame atomic absorption spectrophotometery. Sci J Forensic Med Iri. 2004;9:176–9. [Google Scholar]
- 32.Moharari RS, Khajavi MR, Panahkhahi M, Mojtahedzadeh M, Najafi A. Loss of consciousness secondary to lead poisoning – Case reports. Middle East J Anaesthesiol. 2009;20:453–5. [PubMed] [Google Scholar]
- 33.Narang AP, Chawla LS, Khurana SB. Levels of arsenic in Indian opium eaters. Drug Alcohol Depend. 1987;20:149–53. doi: 10.1016/0376-8716(87)90064-0. [DOI] [PubMed] [Google Scholar]
- 34.Wijesekera AR, Henry KD, Ranasinghe P. The detection and estimation of (A) arsenic in opium, and (B) strychnine in opium and heroin, as a means of identification of their respective sources. Forensic Sci Int. 1988;36:193–209. doi: 10.1016/0379-0738(88)90143-0. [DOI] [PubMed] [Google Scholar]
- 35.Balachandra AT, Balasooriya BA, Athukorale DN, Perera CS, Henry KD. Chronic arsenic poisoning in opium addicts in Sri Lanka. Ceylon Med J. 1983;28:29–34. [PubMed] [Google Scholar]
- 36.Datta DV. Arsenic adulteration in opium. (Arsenicosis – A real danger to health in developing countries) J Assoc Physicians India. 1978;26:223–7. [PubMed] [Google Scholar]
- 37.Antonini G, Palmieri G, Millefiorini E, Spagnoli LG, Millefiorini M. Lead poisoning during heroin addiction. Ital J Neurol Sci. 1989;10:105–8. doi: 10.1007/BF02333882. [DOI] [PubMed] [Google Scholar]
- 38.Algora M, Martín-Castillo A, Zabala P, Fernández MN. Lead poisoning due to drug addiction: A new source of poisoning with clinical interest and important epidemiological consequences. An Med Interna. 1989;6:483–5. [PubMed] [Google Scholar]
- 39.Parras F, Patier JL, Ezpeleta C. Lead-contaminated heroin as a source of inorganic-lead intoxication. N Engl J Med. 1987;316:755. doi: 10.1056/NEJM198703193161217. [DOI] [PubMed] [Google Scholar]
- 40.Questel F, Dugarin J, Dally S. Thallium-contaminated heroin. Ann Intern Med. 1996;124:616. doi: 10.7326/0003-4819-124-6-199603150-00024. [DOI] [PubMed] [Google Scholar]
- 41.Afshari R, Mégarbane B, Zavar A. Thallium poisoning: One additional and unexpected risk of heroin abuse. Clin Toxicol (Phila) 2012;50:791–2. doi: 10.3109/15563650.2012.713110. [DOI] [PubMed] [Google Scholar]