
Fig. 2. The rapidly inactivating ICa is carried by the L-type Ca2+ channels and not by T-type.
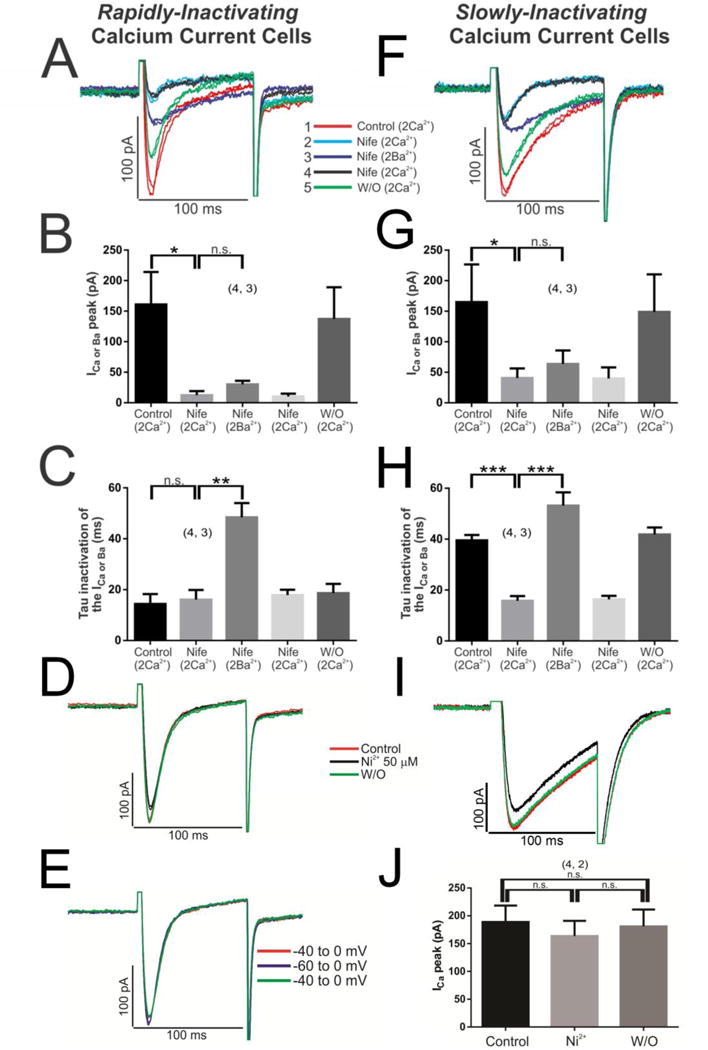
Initially the cells with rapidly inactivating ICa were perfused with 3 μM nifedipine (blue line-Nife, 2 Ca2+), which reduced almost all of the ICa signal (Panels A, B); then the perfusion solution was changed with 2 mM Ba2+ (instead of Ca2+) maintaining the drug nifedipine (purple line-Nife, 2 Ba2+) which in turn modified the τi of the IBa (Panels A, C); the subsequent return to the previous nifedipine-Ca2+ solution (black line-Nife, 2 Ca2+) again reverses the characteristics of the ICa (Panels A–C). The same set of experiments was conducted in cells with slowly inactivating ICa (Panels F–H). 50 μM Ni2+ was used to block T-type calcium channels in rN-CMs with rapidly (Panel D) or slowly inactivating ICa (Panel I). Panel E, shift of the voltage depolarization −40 to −60 mV to recruit possible T-type calcium channels. The duration of each different experimental conditions was 100 s with nifedipine, where the wash/out was extended for 2–3 minutes, nickel where the steady-state was reached in 30 seconds or the experiments with different holding potential (−40/−60 mVs) where the protocol extended only by 15 s.