

Abstract
Background:
Psoriasis is one of the most common skin disorders with a prevalence rate of 0.1%–3%. Chronic nature, frequent relapses, absence of permanent cure, and the cosmetic disfigurement of psoriasis have a negative impact on quality of life (QoL) by causing psychological stress. Patients with psoriasis often have unambiguous ideas about the causes, controllability, consequences, and expected time-course of their disease.
Aim:
The aim of this study is to assess the effectiveness of a video-assisted teaching program regarding psoriasis on the level of knowledge and relaxation therapy on QoL among patients with psoriasis.
Materials and Methods:
Experimental design was adapted. One hundred and four participants diagnosed with psoriasis were randomly allocated either to an experimental or to a control group. Fifty-two participants were included in each group by simple random sampling. A video-assisted teaching program on psoriasis and relaxation exercises was taught to the participants over a period of 3 months. The tools used were: Psoriasis Knowledge Assessment Questionnaire, modified psoriasis disability index, and modified psoriasis life stress inventory.
Results:
In the experimental group, the knowledge score was increased significantly from 9 ± 2.2 at baseline to 23.6 ± 1.5 after the intervention. The disability score was decreased from 15.6 to 9.9 and the stress score related to the illness was decreased from 22.8 to 16.9 after the intervention.
Conclusion:
Educational intervention about disease process and relaxation exercises was effective in improving the knowledge and QoL of patients with psoriasis.
Keywords: Knowledge, psoriasis, quality of life
Introduction
Psoriasis is a chronic inflammatory hyperproliferative disease of the skin and currently affects approximately 0.6% to 4.8% of the world's population.[1] In India, the overall incidence of psoriasis has been reported to be 1.02%.[2] In addition to the skin and joint manifestations, psoriasis impairs many aspects of individual well-being, including emotional, physical, sexual, and financial status.[3] Further, many of the difficulties experienced by patients with psoriasis make demands that outstrip the coping measures of patient and their family or social network. They need sufficient education and support from the health-care providers to manage their condition effectively.[4] This study aimed to assess the effectiveness of a video-assisted teaching program regarding psoriasis on the level of knowledge and relaxation therapy on quality of life (QoL) among patients with psoriasis.
Materials and Methods
Before commencing the study, approval was obtained from Institute Ethics Committee for human studies of the institute, where the study was conducted. Participants signed the written informed consent after being explained about the study. Privacy was provided to the participants and confidentiality was maintained throughout the study. An experimental research design was used to select the sample of 104 participants diagnosed with psoriasis who attended the inpatient and outpatient units of the department of dermatology at a tertiary care hospital. Sample size was estimated using the statistical formula for comparing two related means. The expected change in the mean score of psoriasis life stress inventory (PLSI) as an impact of intervention was 4 with a standard deviation (SD) of 10, and the sample size was estimated at 5% level of significance and 80% power. The samples were selected using simple random sampling. The list of patients registered in the psoriasis clinic was considered. A total of more than 200 patients were undergoing treatment in the psoriasis clinic. The estimated sample size for the study was 51 in each group. The samples were selected using random numbers generated through computer. Patients of both sexes, 18–65 years of age, and with the body surface area involvement of >10% were included in the study. Irrespective of patient's disease status and treatment status, patients were recruited. Participants with acute illness and those who had the diagnosis of any psychiatric disorder were excluded from the study. No participant was found to have psychiatric illness as per clinical evaluation.
Psoriasis knowledge assessment questionnaire
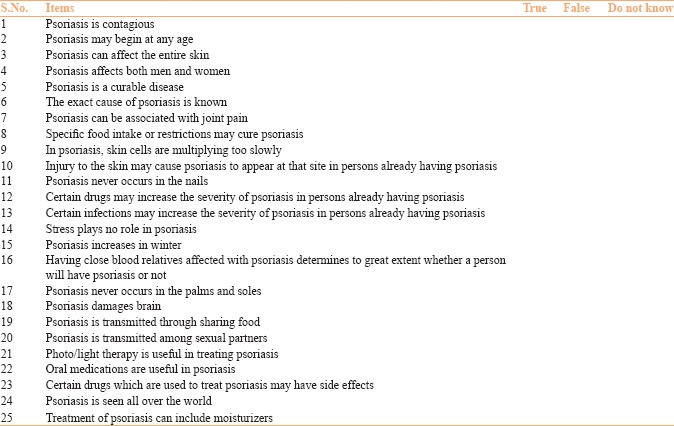
A closed-ended questionnaire was developed to assess the knowledge regarding psoriasis. It consisted of 25 statements pertaining to basic facts on psoriasis (nine items), triggering factors (five items), treatment aspects (four items), and knowledge related to disease process (seven items). The study participants were requested to give “true, false, or do not know” responses. The score ranged from 0 to 25. Reliability coefficient (Cronbach's alpha) was ranged from 0.80 to 0.86. Content validity and face validity were established by the experts from the field of dermatology, psychiatry, and psychology (documented in Appendix I).
Modified psoriasis disability index
The original psoriasis disability index (PDI)[5] is a 15-item validated self-administered questionnaire designed to quantify the functional disability in the aspects of daily activities, employment, personal relationships, leisure, and treatment effects in participants with psoriasis. The score ranged from 0 to 45. The higher the score, the more the QoL is impaired.
In the modified PDI, two questions were added since it would be appropriate for the patients with psoriasis in our specific cultural context: (1) “How is your work in kitchen affected by this condition?” and (2) “How much did the patient experience financial burden due to the treatment of psoriasis?” (Under the subdivisions of work or school and treatment-related questions, respectively). The resulting score thus ranged from 0 to 51 instead of 0–45. The necessary permission was obtained from the authors to use the questionnaire. The modified version of PDI was adapted for the present study from the published literature.
Modified psoriasis life stress inventory
The original 15-item version of PLSI[6] was developed to assess the stress associated with potential psoriasis-related psychosocial problems. The score ranged from 0 to 45. The higher the score the more the QoL is impaired.
In the present study, the stress experienced by the participants was assessed by the modified PLSI which was an 18-item questionnaire. It was found one question – “sunbathing in the company of others”– inappropriate, when applied to our patients and was deleted. Further, four questions were added – feeling less sexually attractive, concerned about children developing psoriasis, fear of relapse, and difficulty in coping if no family support. Thus, the resulting score ranged from 0 to 54 instead of 0–45. Modified version of PLSI was adapted from the literature that was already available.
Statistical analysis
The data were analyzed using both descriptive and inferential statistics using SPSS version 19.0 (IBM Corp. Released 2010. Armonk, NY). The data for the categorical variables on the sociodemographic factors were expressed as frequency and percentage. To calculate the responses in the individual items in knowledge, PLSI, and PDI questionnaire, frequency and percentage were used. The overall scores in knowledge, PLSI, and PDI were expressed as mean with SD. The comparisons of the categorical data between the groups were carried out using Chi-square test. The changes in the level of knowledge, PLSI, and PDI scores over time in each group were analyzed using two-way repeated measures of analysis of variance with repeated contrast test. All statistical analyses were carried out at 5% level of significance, and P < 0.05 was considered as statistically significant.
Data collection procedure
A pretest was conducted by the principal investigator for all the participants in the experimental group as well as in the control group to assess their knowledge on psoriasis and their QoL using modified PDI and modified PLSI. All the participants in the control group received routine dermatological treatment for 12 weeks. All the participants in the experimental group received routine dermatological treatment along with video-assisted teaching program on psoriasis and progressive muscle relaxation exercises along with deep breathing exercises and were followed every week for over 12 weeks. Three posttests were conducted for both the groups with the same questionnaires which were used for pretest at different time points (at the end of 4th, 8th, and 12th week).
Video-assisted teaching program on psoriasis
A video-teaching program was prepared with the details regarding the nature of psoriasis, clinical types, triggering factors, and the diagnostic methods. It also included the description on medications and ointments that are used for the treatment of psoriasis. The side effects of the drugs, precautions to be followed while using ointments, and the signs and symptoms to be reported while taking the drugs were discussed with the participants. The participants were explained about phototherapy and photochemotherapy, and orientation was given to the phototherapy room. Skin care measures and the coping skills were also discussed. Sessions were conducted for four consecutive days and then continued for 12 weeks for reinforcement. An educational pamphlet was provided at the end of the session to reinforce their knowledge.
Jacobson's progressive muscle relaxation technique
The participants in the experimental group were divided into small groups with five in each group and were trained to learn breathing techniques as well as the relaxation techniques. After gaining mastery of relaxation, they were given a regular practice for the period of 12 weeks and the practice was observed by the researcher.
Results
The results of Chi-square analysis showed that there was no significant difference between the groups with respect to demographic variables and the groups were comparable. Comparison of the participants’ knowledge and QoL scores before intervention between the groups is given in Table 1. The change in the mean knowledge score at different time points as an impact of intervention in the experimental group is depicted in Figure 1. The corresponding change of knowledge score in the control group is also depicted in the same figure by line diagram. In the experimental group, the knowledge level was found to be 9.0 before intervention. It was increased to 18.5, 23.2, and 23.6, respectively, at the 1st, 2nd, and 3rd month after the intervention. Similarly, in the control group, the knowledge level was found to be 9.7 before intervention. It was increased to 10.9, 11.3, and 11.4, respectively, at the 1st, 2nd, and 3rd month.
Table 1.
Comparison of the participants’ knowledge and quality of life before intervention (n=104)
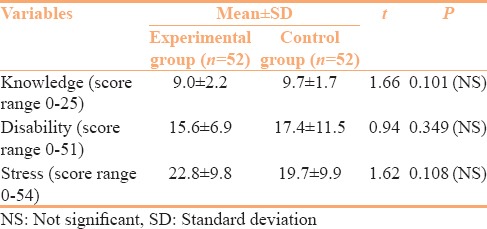
Figure 1.
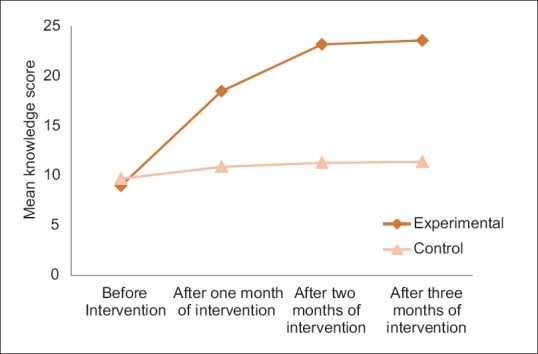
Mean knowledge scores at different time points between the groups (n = 104)
Effectiveness of intervention on disability related to various domains of psoriasis disability index in the experimental group
PDI measures illness-related disability in five aspects, i.e. daily activities, work, personal relations, leisure, and treatment.
The mean PDI score in the experimental group was significantly (P < 0.001) decreased from 15.6 (±6.9) at baseline to 9.9 (±5.1) after 3 months of intervention [Figure 2]. The mean disability score related to daily activities was significantly (P < 0.001) decreased from 5.5 (±3.1) at baseline to 3.6 (±1.7) after 3 months of intervention. The mean disability score related to work was significantly (P < 0.001) decreased from 3.9 (±2.8) at baseline to 2.4 (±1.4); the mean disability score related to personal relations was significantly (P < 0.001) decreased from 1.8 (±1.7) at baseline to 1.3 (±1.3); the mean disability score related to leisure time activities was significantly (P < 0.001) decreased from 2.4 (±1.9) at baseline to 1.4 (±1.4); the mean disability score related to treatment was significantly (P < 0.001) decreased from 2.1 (±1.4) at baseline to 1.4 (±0.8) after the intervention.
Figure 2.
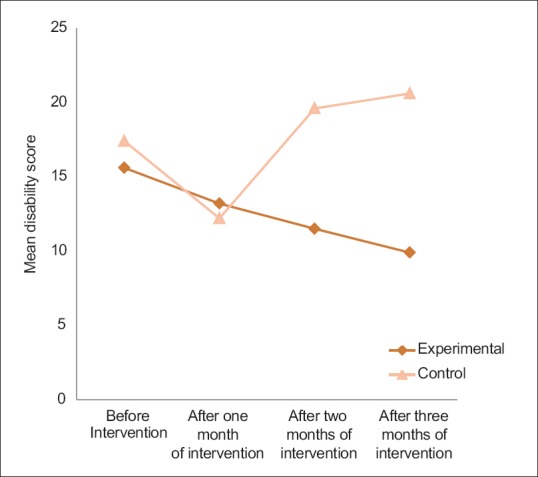
Mean disability (psoriasis disability index) scores at different time points between the groups (n = 104)
The mean PLSI scores in the experimental group were significantly (P < 0.001) decreased from 22.8 (±9.8) at baseline to 16.9 (±6.7) after 3 months of intervention [Figure 3]. Thus, the results of the study suggested that the scores were significant at P < 0.001 level when compared with the control group.
Figure 3.
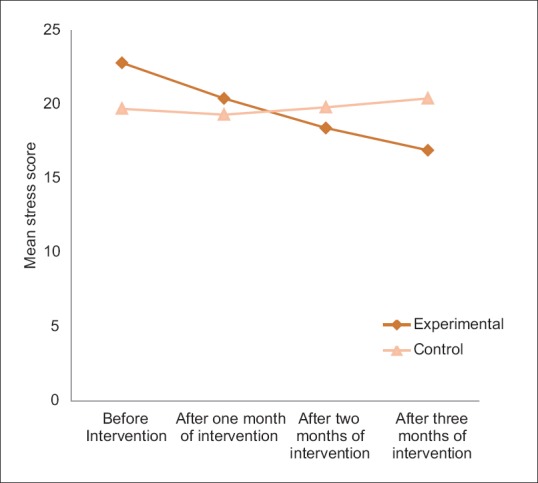
Mean stress scores (psoriasis life stress inventory) at different time points between the groups (n = 104)
Discussion
Many researchers have found that patient's attitudes, knowledge, and behavior toward their disease have a profound effect on its course and severity. For example, a patient with psoriasis who knows about the Koebner phenomenon will be able to avoid injury to the skin. Furthermore, patients with a good understanding of their disease are more self-motivated by increasing their sense of control. Many research findings indicate that it is important to educate patients with psoriasis regarding their condition.[4,7] The results of the present study revealed that the knowledge level was significantly increased in the experimental group due to the impact of the educational program. Similarly, research studies[8,9,10,11] had reported that education and demonstration of topical therapies by specialist dermatology nurses were found to be effective in reducing the severity of clinical symptoms in patients with psoriasis. Other studies which support our study findings are given below:
Wahl et al. investigated patients’ knowledge regarding psoriasis before and after patient education in the context of climate therapy. The authors found significant improvement in the knowledge score immediately after the intervention and 3 months after the intervention when compared to the baseline scores.[12]
Balato et al. evaluated the use of mobile phone-based interventions in improving treatment adherence among twenty patients with psoriasis. The intervention group reported a significantly better improvement of disease severity as well as adherence to therapy in a statistically significant way whereas the control group remained stable.[11]
Bostoen et al. assessed the effect of an educational program on disease severity and QoL in patients with psoriasis or atopic dermatitis. It was found that disease severity and QoL improved significantly for patients with psoriasis after the intervention.[13]
Pagliarello et al. evaluated the effect of a single 2-h empowerment-based educational program in a spa setting at Italy. The experimental group reported higher levels of empowerment with improved knowledge about the disease as compared to the control group.[14] Lora et al. investigated the efficacy of an educational intervention for patients with psoriasis in improving disease knowledge and attitude toward physicians and systemic treatments. The intervention consisted of information on psoriasis and its treatment. After 6 months, a better knowledge about the disease and a better attitude to treatment were retained. It is clearly evident that a single educational intervention may be helpful in improving psoriasis knowledge and give psychological relief to patients.[15]
Werfel et al. conducted an educational program for the management of psoriasis. Five 2-h classes focused on topics relevant for the patients and the management of the disease by dermatologists, psychotherapists/psychologists, and dieticians. This program was accepted very well and seen as helpful by the concerned.[16]
It has long been acknowledged that the clients affected with psoriasis may benefit greatly from psychotherapeutic interventions. It is possible that stress management through relaxation may result in improvement in these patients. Stress may worsen psoriasis severity and may even lengthen the time to disease clearance. According to Zachariae et al.,[17] 66% of their patients reported that their psoriasis was exacerbated by stress and 35% of them reported that the onset of their psoriasis occurred during a time of worry and stress. Rakhesh et al.[18] reported that psoriasis sufferers were most likely to feel self-conscious, disturbed/inconvenienced by the shedding of the skin, lived in a constant fear of relapse, and avoided social interactions.
The findings of the present study showed that the stress score related to the illness was found to be 22.8 before the intervention in the experimental group. It was decreased to 20.4, 18.4, and 16.9, respectively, at the 1st, 2nd, and 3rd month after the intervention due to the impact of educational and relaxation therapy. Similarly, Kabat-Zinn et al.[19] found that meditation-based stress reduction intervention increased the rate of resolution of psoriatic lesions in patients undergoing phototherapy or photochemotherapy treatment. Price et al.[20] reported that patients with psoriasis who were taught specific relaxation techniques had a significant reduction in their anxiety level and showed physical improvement. The present study findings were also supported by the findings of Gaston et al.[9] and Malhotra and Mehta.[21]
Fortune et al. investigated the effects of a cognitive-behavioral psoriasis symptom management program (PSMP) on patient-held perceptions about their condition. Results suggested that at 6-month follow-up, patients who had undergone PSMP showed significant reductions in illness severity.[22]
Ersser et al.[23] searched the literature to assess the effectiveness of psychological and educational interventions in changing outcomes for children with atopic eczema. Four studies focused on intervention directed toward the parents and examined the effect of relaxation techniques (hypnotherapy and biofeedback) on severity. Three educational studies identified significant improvements in disease severity between intervention groups. One study found that video-based education was found to be more effective in improving severity than direct education and the control (P < 0.001). The single psychological study found relaxation techniques resulted in reducing the clinical severity as compared to the control at 20 weeks.
Price et al.[20] investigated whether psychotherapy helps patients with psoriasis. Participants who were taught specific relaxation techniques for use whenever they felt under stress had significantly reduced anxiety level at the end of the study with the modest trend toward physical improvement. No such changes were seen in a matched control group.
Conclusion
The central and peripheral nervous systems, as well as the endocrine system, play an important role in the pathogenesis of psoriasis. Endogenous factors, such as stress, and exogenous factors, such as trauma, cause an increased release of neuropeptides such as substance P. Thus, as a result of stress playing such a prominent role in psoriasis, it seems evident that stress reduction programs should be considered when trying to treat the condition. The results of the present study also suggest that an educational intervention may be helpful in improving the knowledge and give psychological relief to patients with psoriasis.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgement
We sincerely thank Dr. Andrew Finlay for granting us permission to use Psoriasis disability Index and Dr. Gupta MA and Gupta AK for granting us permission to use psoriasis life stress inventory in our research study. We also thank Dr. Malathy M, Assistant Professor, Department of Dermatology, Jawaharlal Institute of Postgraduate Medical Eduation and Research, Puducherry, India.
Appendix 1: Psoriasis Knowledge Assessment Questionnaire
References
- 1.Gelfand JM, Stern RS, Nijsten T, Feldman SR, Thomas J, Kist J, et al. The prevalence of psoriasis in African Americans: Results from a population-based study. J Am Acad Dermatol. 2005;52:23–6. doi: 10.1016/j.jaad.2004.07.045. [DOI] [PubMed] [Google Scholar]
- 2.Jawahar S, Harikrishnan R, Selvarani T, Karthikeyaprabhu B, Somasundaram SS, Thenmozhi K. Prevalence of psoriasis linked to pesticide use in farmers. Int J Pharma World Res. 2011;2:1–23. [Google Scholar]
- 3.Choi J, Koo JY. Quality of life issues in psoriasis. J Am Acad Dermatol. 2003;49:S57–61. doi: 10.1016/s0190-9622(03)01136-8. [DOI] [PubMed] [Google Scholar]
- 4.Jankowiak B, Krajewska-Kulak E, Van Damme-Ostapowicz K, Wronska I, Lukaszuk C, Niczyporuk W, et al. The need for health education among patients with psoriasis. Dermatol Nurs. 2004;16:439–44. [PubMed] [Google Scholar]
- 5.Finlay AY, Coles EC. The effect of severe psoriasis on the quality of life of 369 patients. Br J Dermatol. 1995;132:236–44. doi: 10.1111/j.1365-2133.1995.tb05019.x. [DOI] [PubMed] [Google Scholar]
- 6.Gupta MA, Gupta AK. The psoriasis life stress inventory: A preliminary index of psoriasis-related stress. Acta Derm Venereol. 1995;75:240–3. doi: 10.2340/0001555575240243. [DOI] [PubMed] [Google Scholar]
- 7.Lanigan SW, Layton A. Level of knowledge and information sources used by patients with psoriasis. Br J Dermatol. 1991;125:340–2. doi: 10.1111/j.1365-2133.1991.tb14168.x. [DOI] [PubMed] [Google Scholar]
- 8.Rothman AI, Byrne N, Schachter RK, Rosenberg L, Mitchell D. An educational program for psoriatics: An evaluation. Eval Health Prof. 1980;3:191–203. doi: 10.1177/016327878000300205. [DOI] [PubMed] [Google Scholar]
- 9.Gaston L, Crombez JC, Lassonde M, Bernier-Buzzanga J, Hodgins S. Psychological stress and psoriasis: Experimental and prospective correlational studies. Acta Derm Venereol Suppl (Stockh) 1991;156:37–43. [PubMed] [Google Scholar]
- 10.Cork MJ, Britton J, Butler L, Young S, Murphy R, Keohane SG, et al. Comparison of parent knowledge, therapy utilization and severity of atopic eczema before and after explanation and demonstration of topical therapies by a specialist dermatology nurse. Br J Dermatol. 2003;149:582–9. doi: 10.1046/j.1365-2133.2003.05595.x. [DOI] [PubMed] [Google Scholar]
- 11.Balato N, Megna M, Di Costanzo L, Balato A, Ayala F. Educational and motivational support service: A pilot study for mobile-phone-based interventions in patients with psoriasis. Br J Dermatol. 2013;168:201–5. doi: 10.1111/j.1365-2133.2012.11205.x. [DOI] [PubMed] [Google Scholar]
- 12.Wahl AK, Moum T, Robinson HS, Langeland E, Larsen MH, Krogstad AL, et al. Psoriasis patients’ knowledge about the disease and treatments. Dermatol Res Pract. 2013;2013:921737. doi: 10.1155/2013/921737. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Bostoen J, Bracke S, De Keyser S, Lambert J. An educational programme for patients with psoriasis and atopic dermatitis: A prospective randomized controlled trial. Br J Dermatol. 2012;167:1025–31. doi: 10.1111/j.1365-2133.2012.11113.x. [DOI] [PubMed] [Google Scholar]
- 14.Pagliarello C, Calza A, Armani E, DI Pietro C, Tabolli S. Effectiveness of an empowerment-based intervention for psoriasis among patients attending a medical spa. Eur J Dermatol. 2011;21:62–6. doi: 10.1684/ejd.2010.1197. [DOI] [PubMed] [Google Scholar]
- 15.Lora V, Gisondi P, Calza A, Zanoni M, Girolomoni G. Efficacy of a single educative intervention in patients with chronic plaque psoriasis. Dermatology. 2009;219:316–21. doi: 10.1159/000250826. [DOI] [PubMed] [Google Scholar]
- 16.Werfel T, Breitbart E, Kleinheinz A, Gieler U, Schmid-Ott G. The educational program for the management of psoriasis vulgaris according to the rules of the task force on dermatological prevention: Current status. Hautarzt. 2006;57:913–6. doi: 10.1007/s00105-006-1207-7. [DOI] [PubMed] [Google Scholar]
- 17.Zachariae R, Oster H, Bjerring P, Kragballe K. Effects of psychologic intervention on psoriasis: A preliminary report. J Am Acad Dermatol. 1996;34:1008–15. doi: 10.1016/s0190-9622(96)90280-7. [DOI] [PubMed] [Google Scholar]
- 18.Rakhesh SV, D’Souza M, Sahai A. Quality of life in psoriasis: A study from South India. Indian J Dermatol Venereol Leprol. 2008;74:600–6. doi: 10.4103/0378-6323.45101. [DOI] [PubMed] [Google Scholar]
- 19.Kabat-Zinn J, Wheeler E, Light T, Skillings A, Scharf MJ, Cropley TG, et al. Influence of a mindfulness meditation-based stress reduction intervention on rates of skin clearing in patients with moderate to severe psoriasis undergoing phototherapy (UVB) and photochemotherapy (PUVA) Psychosom Med. 1998;60:625–32. doi: 10.1097/00006842-199809000-00020. [DOI] [PubMed] [Google Scholar]
- 20.Price ML, Mottahedin I, Mayo PR. Can psychotherapy help patients with psoriasis? Clin Exp Dermatol. 1991;16:114–7. doi: 10.1111/j.1365-2230.1991.tb00319.x. [DOI] [PubMed] [Google Scholar]
- 21.Malhotra SK, Mehta V. Role of stressful life events in induction or exacerbation of psoriasis and chronic urticaria. Indian J Dermatol Venereol Leprol. 2008;74:594–9. doi: 10.4103/0378-6323.45100. [DOI] [PubMed] [Google Scholar]
- 22.Fortune DG, Richards HL, Kirby B, Bowcock S, Main CJ, Griffiths CE, et al. A cognitive-behavioural symptom management programme as an adjunct in psoriasis therapy. Br J Dermatol. 2002;146:458–65. doi: 10.1046/j.1365-2133.2002.04622.x. [DOI] [PubMed] [Google Scholar]
- 23.Ersser SJ, Latter S, Sibley A, Satherley PA, Welbourne S. Psychological and educational interventions for atopic eczema in children. Cochrane Database Syst Rev. 2007;3:CD004054. doi: 10.1002/14651858.CD004054.pub2. [DOI] [PubMed] [Google Scholar]