

Abstract
Rationale:
A 50-year-old man presented with complete paralysis at the onset of a putaminal hemorrhage.
Patient concerns:
The patient presented with complete paralysis of the left upper and lower extremities (Medical Research Council:0/5).
Diagnoses:
Spontaneous intra crebral hemorrhage on putamen.
Intervention:
He underwent comprehensive rehabilitative therapy from 3 weeks after onset. At 3weeks after onset, he presented with severe weakness of the left extremities. The weakness of his left extremities had recovered as follows at 3 months after onset. Consequently, he was able to walk independently on an even floor.
Outcomes:
On 3-week and 3-month diffusion tensor tractography (DTTs), the right corticospinal tract (CST) and the corticoreticulospinal tract (CRT) showed discontinuations below the lesion. On 3-month DTT, the left CST had become thinner; however, the left CRT had become thicker compared with 3-week DTT (Fig. 1).
Lessons:
To the best of our knowledge, this is the first study to demonstrate the activation process of the CRT in the unaffected hemisphere in relation to gait recovery from early to chronic stage of stroke.
Keywords: corticoreticulospinal tract, corticospinal tract, diffusion tensor tractography
1. Introduction
A 50-year-old man presented with complete paralysis of the left upper and lower extremities (Medical Research Council: 0/5) at the onset of a putaminal hemorrhage. He underwent comprehensive rehabilitative therapy from 3 weeks after onset. At 3 weeks after onset, he presented with severe weakness of the left extremities (shoulder abductor; 0, elbow flexor: 0, finger extensors; 0, hip flexor; 1, knee extensor; 3- and ankle dorsiflexor; 2-). The weakness of his left extremities had recovered as follows at 3 months after onset (shoulder abductor; 2+, elbow flexor: 4−, finger extensor; 0, hip flexor; 4−, knee extensor; 4+ and ankle dorsiflexor; 2−). Consequently, he was able to walk independently on an even floor.
Diffusion tensor tractography (DTT) data were acquired twice at 3 weeks and 3 months after onset. On 3-week and 3-month DTTs, the right corticospinal tract (CST) and the corticoreticulospinal tract (CRT) showed discontinuations below the lesion. On 3-month DTT, the left CST had become thinner; however, the left CRT had become thicker compared with 3-week DTT (Fig. 1). This study was conducted retrospectively, and the study protocol was approved by the institutional review board of our university hospital.
Figure 1.
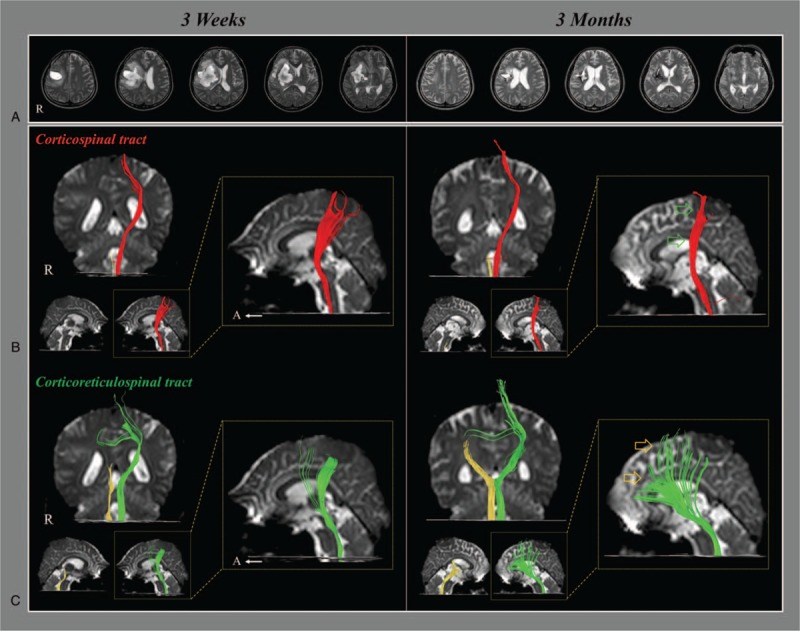
(A) T2-weighted magnetic resonance images show a putaminal hemorrhage in the right hemisphere at 3 weeks and 3 months after onset. (B) Result of diffusion tensor tractography (DTT), the right corticospinal tract (CST) shows discontinuation at the brainstem on both 3-week and 3-month DTT. By contrast, on 3-month DTT, the left CST has become thinner (green arrow) compared with 3-week DTT. (C) The right corticoreticulospinal tract (CRT) shows discontinuation below the lesion on both 3-week and 3-month DTT. On 3-month DTT, the left CRT has become thicker (yellow arrow) compared with 3-week DTT.
The CRT, which mainly controls proximal and axial muscles, is known to have a major role in gait function.[1,2] In this patient, it appears that the motor function of the left (affected) extremities and gait function were mainly attributed to the activation of the left CRT, for the following reasons. His motor function of the left extremities and gait function recovered slowly during approximately 2 month's rehabilitation from 3 weeks to 3 months after onset. The motor recovery occurred mainly in the proximal and leg muscles, which are responsible for the CRT.[1,3] Among 2 important motor tracts, only the left (unaffected) CRT became thickened, whereas the left CST became thinner without significant change of the right (affected) CST and CRT. These results appear to coincide with those of the previous study, which demonstrated that the gait function of chronic stroke patients who showed complete injury of the CST and CRT was related to increased fiber number of the unaffected CRT.[4] Consequently, to the best of our knowledge, this is the first study to demonstrate the activation process of the CRT in the unaffected hemisphere in relation to gait recovery from early to chronic stage of stroke.
Footnotes
Abbreviations: DTT = diffusion tensor tractography, CST = corticospinal tract, CRT = corticoreticulospinal tract.
This work was supported by the National Research Foundation(NRF) of Korea Grant funded by the Korean Government(MSIP) (2015R1A2A2A01004073).
The authors report no conflicts of interest.
References
- [1].Mendoza JE, Foundas AL. Clinical neuroanatomy: a neurobehavioral approach. New York; London: Springer; 2007. [Google Scholar]
- [2].Miyai I, Yagura H, Oda I, et al. Premotor cortex is involved in restoration of gait in stroke. Ann Neurol 2002;52:188–94. [DOI] [PubMed] [Google Scholar]
- [3].Yeo SS, Chang MC, Kwon YH, et al. Corticoreticular pathway in the human brain: Diffusion tensor tractography study. Neurosci Lett 2012;508:9–12. [DOI] [PubMed] [Google Scholar]
- [4].Jang SH, Chang CH, Lee J, et al. Functional role of the corticoreticular pathway in chronic stroke patients. Stroke 2013;44:1099–104. [DOI] [PubMed] [Google Scholar]