

Abstract
Purpose of Review
In the past several years, there have been significant advances in our understanding of the natural history of rotator cuff disease. Studies have continued to provide valuable insight into the clinical, radiographic, and anatomic features of these atraumatic tears. Our purpose is to summarize the findings and contributions from these recent high-quality studies.
Recent Findings
Current research has continued to describe and provide understanding into the natural history of atraumatic rotator cuff disease, including symptom progression, tear enlargement, and the development of arthritis. This knowledge has allowed identification of tears with higher risk of disease progression. Additionally, studies have investigated, with long-term healing data, whether the natural history of degenerative rotator cuff tears can be altered with surgical intervention.
Summary
Recent studies have shown encouraging mid to long-term healing data and clinical outcome scores for smaller tears in younger patients with minimal fatty infiltration. Future research should focus on obtaining long-term healing data, functional outcome data, and refining surgical indications for rotator cuff repair. Identifying patients with specific tear characteristics amendable to healing will allow us to provide a long-term, durable repair, thus interrupting the natural history of degenerative rotator cuff disease.
Keywords: Natural history, Rotator cuff, Atraumatic, Degenerative, Recent literature
Introduction
Over the last two decades, there has been much research that has helped clinicians better understand the natural history of degenerative rotator cuff disease. These studies, often relying on abnormalities in the asymptomatic shoulder, suggest that atraumatic rotator cuff tears are part of the normal aging process in many individuals [1]. In a systematic review investigating the prevalence of rotator cuff disease with increasing age, Teunis et al. showed that abnormalities ranged from 9.7% in patients aged 20 years and younger and increased to 62% in patients of 80 years and older [2]. This increase persisted regardless of the presence of symptoms.
Patients with unilateral shoulder pain are also at an increasingly age-related greater risk of possessing a rotator cuff tear in their contralateral, asymptomatic shoulder. In a comparative study of patients with unilateral shoulder pain, the average age for a patient without a rotator cuff tear was 48.7 years [3]. The age increased to 58.7 years for a unilateral tear, and 67.8 years for those with a bilateral tear. A 50% likelihood of bilateral tear was shown to be after the age of 66 years. Although age was linked with the presence and type of rotator cuff tear, it was not linked to the size of the tear.
Studies investigating the initiation and propagation of rotator cuff tears have improved our understanding to the pathogenesis of rotator cuff disease. Kim et al., in an analysis of 360 shoulders with partial or full-thickness tears, showed the location of 15 to 16 mm posterior to the biceps tendon to be the most commonly torn location within the posterior cuff tendons (Fig. 1) [4]. Furthermore, the patterns of tear location across multiple tear sizes, generated on frequency histograms, suggest that degenerative cuff tears may initiate in a region 13 to 17 mm posterior to the biceps tendon. From this location, tears then propagate as the disease progresses. This study highlighted to common tear location to be within the rotator crescent often sparing the anterior cable insertion of the supraspinatus. The authors showed that only 30% of full-thickness rotator cuff tears involved the most anterior aspect of the supraspinatus tendon footprint.
Fig. 1.
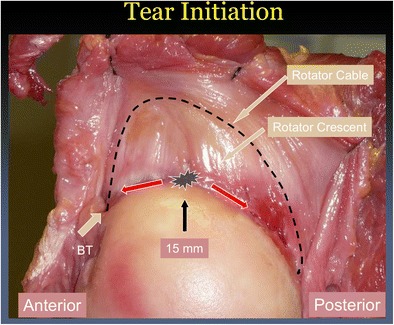
Anatomic description of degenerative rotator cuff tear. The common site of tear location of degenerative cuff tears is 13–17 mm posterior to the biceps tendon within the rotator crescent tissue. BT biceps tendon. Originally from Kim KH, Dahiya N, Teefey SA, Middleton WD, Stobbs G, Steger-May K, Yamaguchi K and Keener JD. Location and initiation of degenerative rotator cuff tears: an analysis of 360 shoulders. J Bone Joint Surg 2010;92:1088–96. Fig. 5, page 1094
Tear size and tear location have been shown to correlate closely with fatty degeneration of rotator cuff muscles. In a study investigating these factors in 413 shoulders, fatty degeneration was seen on ultrasound imaging almost exclusively in full-thickness tears [5]. In shoulders with fatty degeneration, tear length and width were significantly larger. In addition, as the distance measured from posterior to the biceps tendon and to the anterior edge of the rotator cuff tear decreased, the number of fatty infiltrated muscles increased. Regression analysis demonstrated that tear size was the most important predictor of infraspinatus degeneration, whereas disruption of the anterior supraspinatus tendon was the most important predictor of supraspinatus muscle degeneration.
Proximal migration is commonly seen in rotator cuff deficient shoulders via alteration of normal glenohumeral kinematics. It has been shown that the size of the tear correlates strongly with humeral migration and is the strongest predictor of migration in symptomatic shoulders [6]. A tear area threshold of 175mm2 was identified as a critical size, which demonstrated a positive correlation to migration. Smaller tears did not demonstrate significant correlation with migration regardless of the presence or absence of pain. Greater involvement of the infraspinatus leads to significantly greater alteration of glenohumeral kinematics.
On the basis of these and other studies, the natural history of atraumatic rotator cuff disease follows a predictable clinical path. As patients age, asymptomatic full-thickness rotator cuff tears increase in incidence. These tears initiate at the junction of the posterior supraspinatus and anterior infraspinatus within the rotator crescent, propagating from that point. As the tear size increases, the amount of fatty degenerative changes increases, as does the number of muscles involved. Once the tear size progresses to a critical tear threshold, proximal humeral migration is observed. More recent research from the last 3–5 years has focused on continuing to describe and understand the natural history of atraumatic rotator cuff disease, including symptom progression, tear enlargement, and the development of arthritis. Additionally, studies have investigated, with long-term healing data, whether the natural history of atraumatic rotator cuff tears can be altered with surgical intervention.
Recent Advances
Radiographic Studies
In the evaluation of rotator cuff pathology, distinction between tear initiation resulting from trauma and atraumatic degenerative tearing may pose a challenge. In the clinical evaluation of a patient with shoulder pain, a history of trauma may not clearly exist. As the management of acute, traumatic tears can differ from atraumatic, degenerative tears, this distinction is important [7]. Upon analyzing radiography and magnetic resonance imaging (MRI) features of 50 patients with rotator cuff lesions, Loew et al. observed a number of MRI features suggestive of a traumatic etiology [8]. On MRI, edema in the injured muscle and a kinking, wave-like appearance of the central tendon was more suggestive of trauma, while more muscular fatty infiltration was found in the atraumatic group (Fig. 2). Interestingly, thinning and the degree of tendon retraction did not differ between the two groups.
Fig. 2.
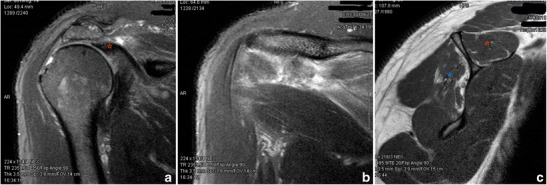
MRI sequences from traumatic rotator cuff tear. a Coronal image—retracted supraspinatus/infraspinatus tendon (red asterisk). b Coronal image—more posterior slice demonstrating edema (fluid signal) throughout infraspinatus muscle. c Sagittal image - grade 2 muscle fatty infiltration noted in the infraspinatus (blue asterisk). The supraspinatus muscle (red asterisk) is healthy.
Another radiographic study investigated acromial morphological characteristics, with a particular focus on the critical shoulder angle (CSA) and its association with rotator cuff disease [9]. In a comparison of longitudinally collected data, 313 patients with asymptomatic rotator cuff tears were evaluated with ultrasound and radiographs annually for a median of 4 years. A second group of 119 patients diagnosed with adhesive capsulitis and normal radiographs served as controls. Only 326 (21%) of 1552 radiographs were of sufficient quality to measure the CSA due to the influence of scapular position on boney landmarks as defined by Suter et al. [10]. Patients with cuff tears had a slightly higher (mean of 2°) CSA, but the CSA was not different between enlarging and stable tears, it did not change over time, and it did not correlate with baseline tear length. The authors concluded that the CSA is unlikely to be related to degenerative rotator cuff disease. The association of CSA and rotator cuff disease continues to be debated as some authors have noted a positive correlation of rotator cuff tears with a larger CSA [11–13].
Tear Progression and Pain Development
It has been well established that there is a time-dependent risk of tear enlargement in shoulders with degenerative rotator cuff tears. Examination of the natural history of cuff disease may be best performed in asymptomatic tears where no treatment, which may influence tear progression, is necessary. Keener et al. prospectively studied 224 asymptomatic shoulders over a median 5.1 years with an asymptomatic rotator cuff tear in one shoulder and contralateral pain due to rotator cuff disease [14••]. Tear enlargement was seen in 49% of shoulders at a median 2.8 years. Through the duration of the study, 46% of shoulders developed new pain. Full-thickness tears progressed in size, became symptomatic, and demonstrated progression of muscle degeneration more frequently than partial-thickness tears and normal controls. The 2 and 5-year risk of tear enlargement were 11 and 35% for partial tears compared to 22 and 50% for full-thickness tears. Tear enlargement was also associated with hand dominance suggesting that activity level may play a role in tear progression. The presence of tear enlargement was associated with new pain in all tear types; however, this relationship was not absolute (hazard ratio of 1.66). Currently, the factors most responsible for pain development in shoulders with asymptomatic tears have not been clearly defined.
Recent research has more closely examined patterns of tear progression for degenerative rotator cuff tears. Regarding tear propagation, 139 asymptomatic tears followed for a median of 6 years were classified based on the integrity of the anterior 3 mm (rotator cable) of the supraspinatus tendon [15]. These rotator cable-intact tears propagated by ultrasound bidirectionally (median of 5 mm anteriorly and 4 mm posteriorly), while cable-disrupted tears propagated a median of 7 mm posteriorly. There was no difference in risk of enlargement or time to enlargement based on the integrity of the anterior supraspinatus (Fig. 3). In small to medium-sized rotator cuff tears, the influence of the integrity of the anterior supraspinatus tendon was evaluated with both patient-reported outcomes and with postoperative ultrasound following surgical repair [16]. Disruption of the anterior supraspinatus tendon in painful small and medium tears was associated with greater tear size and supraspinatus muscle degeneration compared to tears with an intact anterior supraspinatus tendon. However, anterior tendon integrity had no influence on baseline function, postoperative functional parameters, or tendon healing rates.
Fig. 3.
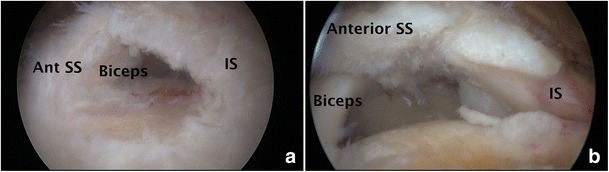
Intraoperative photos of degenerative rotator cuff tears. a Anterior supraspinatus intact tear—note intact cuff fibers posterior to the biceps tendon. SS supraspinatus, IS infraspinatus. b Anterior supraspinatus disrupted tear—uncovering of the biceps tendon due to disruption of the anterior supraspinatus insertion. SS supraspinatus, IS infraspinatus
Patient-related factors such as activity level have been recently examined as a risk factor for tear progression over time. A study of 346 asymptomatic rotator cuff tears over 4.1 years demonstrated that tear enlargement and pain development was more common in the dominant shoulder, yet shoulder activity level and occupational demand were not related to tear progression risks [17•]. Patients with higher occupational demands were more likely to develop pain. Dunn et al., in a cohort of 393 patients with full-thickness rotator cuff tears treated conservatively, showed that the anatomic features defining the severity of atraumatic rotator cuff tears were not associated with pain level [18]. These authors demonstrated that the patient-related factors of medical comorbidities, lower education level, and race rather than tear-related factors were associated with pain severity. Additional studies investigating the risk of rotator cuff tear enlargement are highlighted in Table 1 [14••, 15, 17•, 19–23].
Table 1.
Risk of atraumatic rotator cuff tear progression
| Study | Study demographics | Length of follow-up | Imaging modality | Results |
|---|---|---|---|---|
| Keener et al., JBJS 2015 | 118 asymptomatic patients with full-thickness tears, 56 with partial tears, and 50 controls | Median 5.1 years | Ultrasound | -Tear enlargement occurred in 61% of full thickness, 44% of partial, and 14% of controls -2 and 5-year risk of enlargement in partial tears were 11 and 35% compared to 22 and 50% for full-thickness tears -Enlargement associated with hand dominance, pain development, and cuff muscle degeneration -Enlargement not correlated with size, age, or gender |
| Keener et al., JSES 2015 | 139 asymptomatic full-thickness tears, classified based on integrity of anterior 3 mm of supraspinatus tendon (rotator cable) | Median 6 years | Ultrasound | -Rotator cable-intact tears propagated a median of 5 mm anteriorly and 4 mm posteriorly -Rotator cable-disrupted tears propagated a median 7 mm posteriorly -No difference in risk of enlargement, time to enlargement, or magnitude of enlargement based on rotator cable integrity |
| Keener et al., JSES 2017 | 346 asymptomatic shoulders: 175 full-thickness tears, 103 partial tears, and 68 controls | Median 4.1 years | Ultrasound | -Tear enlargement occurs in 51% -Dominant shoulder had greater risk of enlargement -Shoulder activity level and occupational demand level were not predictive of tear enlargement |
| Maman et al., JBJS 2009 | 49 symptomatic rotator cuff tears | Minimum 6 months | MRI | -Follow-up greater than 18 months associated with greater tear progressions (48 vs 19%) -Age > 60 associated with tear progression (54 vs 17%) -Risk of tear enlargement associated with presence of fatty muscle infiltration |
| Mall et al., JBJS 2010 | 195 asymptomatic rotator cuff tears | 2 years | Ultrasound | -Pain developed in 23% of patients -Pain associated with increase in tear size -With pain development, 18% of full-thickness tears increased > 5 mm, and 40% of partial tears progressed to full-thickness tears |
| Safran et al., AJSM 2011 | 61 symptomatic full-thickness rotator cuff tears in 51 patients aged < 60 years | 2–3 years | Ultrasound | -49% of tears enlarged, 43% were stable in size, and 8% decreased in size -Positive correlation of tear enlargement and pain development -Age, prior trauma, initial tear size, and bilateral tears not associated with tear enlargement |
| Fucentese et al., JBJS 2012 | 24 symptomatic full-thickness rotator cuff tears aged < 65 | Mean 42 months | Initial MR Arthrogram, F/U MRI | -11 patients had no tear or smaller tear at f/u -9 patients had no change in tear size -6 patients (25%) had increased tear size |
| Moosmayer et al., JBJS 2013 | 50 asymptomatic full-thickness tears | 3 years | Ultrasound and MRI | -Painful shoulders had greater enlargement (10.6 vs 3.3 mm) -Increased rate of progression of advanced atrophy (35 vs 12%) and fatty muscle degeneration (35 vs 4%) in painful shoulders |
Fatty Muscle Degeneration
While it has been shown that fatty muscle degeneration is seen almost exclusively in full-thickness tears, the progression of fatty degeneration over time had not previously been studied in the natural history of atraumatic rotator cuff tears. In a study with 156 asymptomatic full-thickness rotator cuff tears followed for a median of 6.0 years, the presence of muscle degeneration was seen in older patients, with larger tears at baseline (13.0 vs 10.0 mm) and in tears that enlarged during follow-up (79 vs 58% that did not enlarge) [24••]. Progression of muscle degeneration, when present, was greater in tears that enlarged compared to stable tears (43 vs 20%). Additionally, progression of muscle degeneration was more frequent in tears that enlarged when the baseline tear size was greater (15.0 vs 10.0 mm), the magnitude of enlargement was greater (9 vs 5 mm), and with disruption of the anterior supraspinatus tendon insertion (53 vs 17%), although this latter relationship was lost when controlling for baseline tear size. The authors noted a wide distribution of the temporal relationship of tear enlargement to the progression of muscle degeneration; however, the median time to progression of muscle changes in relation to tear enlargement was 1.0 year for the supraspinatus and 1.1 years for the infraspinatus.
Arthritis Progression
Until recently, little information regarding the risks of progression of radiographic cuff tear arthropathy in untreated rotator cuff tears was unknown. Over an average 8-year period, Chalmers et al. showed significant progression of glenohumeral arthritic changes in shoulders with a wide range of cuff tear severity, although these changes remained minimal [25]. The presence of a cuff tear (partial or full thickness) influenced progression in Hamada grade, but the magnitude of radiographic progression did not appear to be influenced by the cuff tear size or cuff tear enlargement. Although advancing proximal humeral migration was seen in some shoulders, it is important to note that severe arthritic changes were rarely seen over this 8-year timeframe.
Nonoperative Management
Debate exists among providers regarding how atraumatic rotator cuff tears are best managed clinically. One large database study investigated treatment modality trends in Medicare patients over an 8-year period in patients diagnosed with a rotator cuff tear [26]. Overall, they found a decrease in the utilization of initial nonoperative treatment modalities and a corresponding rise in rate of surgery. The proportion of patients treated initially with therapy decreased from 30% in 2005 to 13.2% in 2012. The use of subacromial and glenohumeral injections decreased from 6.0 to 4.2%, while the rate of surgery increased from 33.8 to 40.4%. Those patients undergoing repair had a significantly lower Charlson comorbidity index.
The MOON Shoulder Group, in a multicenter study, evaluated predictors of failure of nonoperative treatment of chronic, symptomatic, full-thickness rotator cuff tears [27•]. Tear characteristics and the severity of shoulder pain and weakness did not predict failure of the nonoperative group. Instead, the strongest predictor of failure was low patient expectations about the effectiveness of physical therapy. Other predictors included activity level and a nonsmoking status.
A long-term study following the natural course of selected rotator cuff tears treated nonoperatively was conducted in 49 shoulders at a mean of 8.8-year follow-up [28••]. In this subgroup of shoulders, variability in tear enlargement was found. The mean tear width increased 8.3 mm; however, one third of shoulders increased more than 10 mm. Progression of degenerative muscle changes to a Goutallier stage 3 or 4 was observed in 41% by MRI at final follow-up. Half of the shoulders progressed from an initially good prognosis for a successful anatomical repair to a poor prognosis. Clinically, the authors found a significant decline in ASES and Constant scores when tear enlargement greater than 20 mm occurred or when progression of muscle degeneration was seen.
Kukkonen et al. performed a randomized controlled trial of shoulders with symptomatic, atraumatic full-thickness supraspinatus tears with 2 years of follow-up [29]. Patients were randomized into one of three treatment groups consisting of either physical therapy, acromioplasty and physical therapy, or rotator cuff repair, acromioplasty, and physical therapy. At follow-up, the authors found no significant differences in the mean change of Constant scores among 167 shoulders in 160 patients. Visual analog pain scales and patient satisfaction were not significantly different among the treatment groups. In another randomized controlled trial in patients with degenerative full-thickness cuff tears, 31 patients were treated nonoperatively, and 25 underwent surgical repair [30]. Differences in functional outcomes measured by the Constant score were not observed at 1 year of follow-up. Differences in VAS pain and disability were significant and in favor of surgical treatment. Surprisingly, the authors reported a retear rate of 73.7% on MRI at follow-up, and concluded that the best outcomes in function and pain were seen in surgically treated patients with an intact cuff repair postoperatively.
Moosmayer et al. performed a randomized control trial comparing nonoperative treatment to surgical repair in 103 shoulders with full-thickness rotator cuff tears less than 30 mm with a minimum of 5 years of follow-up [31••]. Both surgical intervention and physical therapy were successful in treating the tears; however, close to one quarter of the therapy group failed treatment and underwent delayed surgery. Tears managed surgically had significantly better ASES (9 points) and Constant scores (5.3 points) and VAS analog pain scores (1.1) than the shoulders treated with physical therapy. The authors noted declining function and increasing tear size in 37% of shoulder treated with physical therapy. The authors concluded that the beneficial effect of surgery was clinically negligible as the difference between groups did not reach the minimal clinically important difference for the outcome scales.
Healing Data
Successful interruption of the natural history of degenerative rotator cuff disease with surgical intervention is predicated on obtaining a durable repair and consistent clinical results. Previous research has established that the most important variable influencing the rate of tendon healing to be the age of the patient, the tear size, and the severity of fatty muscle degeneration/infiltration. Recent literature has investigated the extent at which variable demographic, anatomic, and radiographic characteristics affect the rate of obtaining a durable surgical repair of atraumatic rotator cuff tears. Park et al. investigating variable prognostic factors affecting healing in small to medium-sized tears [32•]. Overall, they found a 13.3% retear rate on MRI at least 1 year after surgery in 339 patients undergoing arthroscopic repair. They concluded that a tear size of 2 cm is the threshold for healing, noting a 34.2% retear rate for repairs greater than 2 cm vs 10.6% of tears equal to or less than 2 cm. The other independent prognostic factors for poor rotator cuff healing in this study tears were higher grade infraspinatus fatty infiltration (Goutallier grade II or higher) and age greater than 69 years.
The effect of tendon retraction and healing has also been investigated [33]. The authors correlated rotator cuff musculotendinous junction (MTJ) retraction with healing in 51 patients treated by a single-row technique. By referencing the MTJ with respect to the glenoid on preoperative MRI studies compared to postoperative repair integrity, they showed 93% healing with a MTJ lateral to the glenoid face and only 55% healing if medial to the face. Overall, 76% of tears healed, with 87% healing in small/medium tears and 62% healing in large/massive tears.
In a review of 1300 consecutive patients undergoing arthroscopic rotator cuff repair, Tan et al. studied the effect of tear mechanism on tendon healing [34]. A preoperative questionnaire was utilized to identify cohorts of patients with or without a history of trauma on presentation. There was no statistically significant difference in the retear rates of the “no trauma” group (12%) compared to the trauma group (14%) at 6 months postoperatively on ultrasound. However, the patients with a history of trauma who waited longer than 24 months had higher retear rates (20%) that those who had surgery earlier (13%). The overall retear rate was 14%.
Multiple similar studies by the same group have investigated variable factors and their subsequent effect on retear rates. In 1600 consecutive arthroscopic rotator cuff repairs, a low rate of rotator cuff retears was shown in patients less than 50 years old, with a linear retear rate between ages 50 and 69, increasing 5% between decades. Retears increase significantly in patients aged 70 or older [35•]. The overall retear rate was 13% [36]. Significant improvement in pain levels with overhead activity, as well as range of motion with forward flexion and abduction, was seen irrespective of cuff integrity. Repair integrity positively influenced supraspinatus and external rotation power. In another study, smaller tears were shown to have fewer retears (7% in tear size < 2 cm2 vs 44% in tear size > 8 cm2). Patients with smaller tears had more pain during the 6-week to 6-month postoperative period than larger tears [37]. The authors hypothesized a more robust healing response in the smaller tears, leading to more postoperative pain.
In a multicenter study, isolated supraspinatus tears treated surgically were evaluated 10 years postoperatively providing an improved understanding of the durability of rotator cuff repair surgery. Collin et al. reviewed 288 subjects clinically with MRI follow-up on 210 shoulders. [38••]. Subjects had considerable improvement in clinical outcomes that remained durable at 10-year follow-up. The mean Constant score improved from 51.8 preoperatively to 77.7 at final follow-up. The final Constant score was positively associated with an intact repair and inversely associated with preoperative muscular fatty infiltration. Healing was seen in 81% of shoulders at final follow-up.
Future Research
The last half-decade has seen significant advances in our understanding of the natural history of rotator cuff disease. Studies have continued to provide valuable insight into the clinical, radiographic, and anatomic features of these atraumatic tears. Healing data in postoperative patients has allowed us to refine surgical indications based on predictive factors for successful or unsuccessful repair.
One study has provided an algorithm for surgical indications by classifying rotator cuff tears into three categories based on the relative risks of nonoperative management and potential benefits of surgical management [39]. Group I, or the early operative repair group, includes shoulders with a full-thickness tears as a result of a distinct, acute event as well as younger patients (under 62–65 years) with small to medium full-thickness tears with minimal or no atrophy. Given recent natural history data, an increased benefit to early surgical intervention may be amplified if the tear is greater than 15–20 mm in size or when there is disruption of the anterior cable attachment of the supraspinatus. Consideration for early surgical intervention is given based on the established risks of tear enlargement and progression of muscle atrophy in a patient still able to heal the repair. Group II includes partial thickness tears and atraumatic degenerative tears with signs of chronicity. These tears warrant a trial of initial nonoperative management and may respond to surgery if nonoperative management fails. Group III includes tears that are unlikely to heal. Nonoperative treatment should be maximized. These tears include tears in older patients (> 70 years), chronic and retracted full-thickness tears with muscle degeneration, and tears with fixed proximal humeral migration. Conservative treatment should be maximized for these patients.
Future research on the natural history of atraumatic rotator cuff tears should focus on continuing to understand the factors related to pain development, which have remained elusive. Additionally, obtaining long-term healing and functional outcome data as they relate to various stages of rotator cuff disease will allow for refinement of surgical indications for rotator cuff repair.
Conclusions
Our understanding of the natural history of atraumatic rotator cuff disease has grown significantly. Recent studies have shown encouraging mid to long-term healing data and clinical outcome scores for smaller tears in younger patients with minimal fatty infiltration. Larger tears in older patients with advanced stages of fatty infiltration have shown less promising results with attempted surgical repair. Continued study of the natural history and disease progression will lead to more refined surgical indications, thus optimizing outcomes. Identifying patients with specific tear characteristics amendable to healing will allow us to provide a long-term, durable repair, thus interrupting the natural history of atraumatic rotator cuff disease.
Compliance with Ethical Standards
Conflict of Interest
Jason L. Codding declares that he has no conflict of interest.
Jay D. Keener reports grants from the NIH, during the conduct of study.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Footnotes
This article is part of the Topical Collection on Rotator Cuff Repair
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
- 1.Milgrom C, Schaffler M, Gilbert S, van Holsbeeck M. Rotator-cuff changes in asymptomatic adults. The effect of age, hand dominance and gender. J Bone Joint Surg Br. 1995;77(2):296–298. doi: 10.1302/0301-620X.77B2.7706351. [DOI] [PubMed] [Google Scholar]
- 2.Teunis T, Lubberts B, Reilly BT, Ring D. A systematic review and pooled analysis of the prevalence of rotator cuff disease with increasing age. J Shoulder Elb Surg. 2014;23(12):1913–1921. doi: 10.1016/j.jse.2014.08.001. [DOI] [PubMed] [Google Scholar]
- 3.Yamaguchi K, Ditsios K, Middleton WD, Hildebolt CF, Galatz LM, Teefey SA. The demographic and morphological features of rotator cuff disease. A comparison of asymptomatic and symptomatic shoulders. J Bone Joint Surg Am. 2006;88(8):1699–1704. doi: 10.2106/JBJS.E.00835. [DOI] [PubMed] [Google Scholar]
- 4.Kim HM, Dahiya N, Teefey SA, Middleton WD, Stobbs G, Steger-May K, Yamaguchi K, Keener JD. Location and initiation of degenerative rotator cuff tears: an analysis of three hundred and sixty shoulders. J Bone Joint Surg Am. 2010;92(5):1088–1096. doi: 10.2106/JBJS.I.00686. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Kim HM, Dahiya N, Teefey SA, Keener JD, Galatz LM, Yamaguchi K. Relationship of tear size and location to fatty degeneration of the rotator cuff. J Bone Joint Surg Am. 2010;92(4):829–839. doi: 10.2106/JBJS.H.01746. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Keener JD, Wei AS, Kim HM, Steger-May K, Yamaguchi K. Proximal humeral migration in shoulders with symptomatic and asymptomatic rotator cuff tears. J Bone Joint Surg Am. 2009;91(6):1405–1413. doi: 10.2106/JBJS.H.00854. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Petersen SA, Murphy TP. The timing of rotator cuff repair for the restoration of function. J Shoulder Elb Surg. 2011;20(1):62–68. doi: 10.1016/j.jse.2010.04.045. [DOI] [PubMed] [Google Scholar]
- 8.Loew M, Magosch P, Lichtenberg S, Habermeyer P, Porschke F. How to discriminate between acute traumatic and chronic degenerative rotator cuff lesions: an analysis of specific criteria on radiography and magnetic resonance imaging. J Shoulder Elb Surg. 2015;24(11):1685–1693. doi: 10.1016/j.jse.2015.06.005. [DOI] [PubMed] [Google Scholar]
- 9.Chalmers PN, Salazar D, Steger-May K, Chamberlain AM, Yamaguchi K, Keener JD. Does the critical shoulder angle correlate with rotator cuff tear progression? Clin Orthop. 2017;475(6):1608–1617. doi: 10.1007/s11999-017-5249-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Suter T, Gerber Popp A, Zhang Y, Zhang C, Tashjian RZ, Henninger HB. The influence of radiographic viewing perspective and demographics on the critical shoulder angle. J Shoulder Elb Surg. 2015;24(6):e149–e158. doi: 10.1016/j.jse.2014.10.021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Moor BK, Wieser K, Slankamenac K, Gerber C, Bouaicha S. Relationship of individual scapular anatomy and degenerative rotator cuff tears. J Shoulder Elb Surg. 2014;23(4):536–541. doi: 10.1016/j.jse.2013.11.008. [DOI] [PubMed] [Google Scholar]
- 12.Moor BK, Bouaicha S, Rothenfluh DA, Sukthankar A, Gerber C. Is there an association between the individual anatomy of the scapula and the development of rotator cuff tears or osteoarthritis of the glenohumeral joint?: a radiological study of the critical shoulder angle. Bone Jt J. 2013;95–B(7):935–941. doi: 10.1302/0301-620X.95B7.31028. [DOI] [PubMed] [Google Scholar]
- 13.Blonna D, Giani A, Bellato E, Mattei L, Caló M, Rossi R, Castoldi F. Predominance of the critical shoulder angle in the pathogenesis of degenerative diseases of the shoulder. J Shoulder Elb Surg. 2016;25(8):1328–1336. doi: 10.1016/j.jse.2015.11.059. [DOI] [PubMed] [Google Scholar]
- 14.Keener JD, Galatz LM, Teefey SA, Middleton WD, Steger-May K, Stobbs-Cucchi G, Patton R, Yamaguchi K. A prospective evaluation of survivorship of asymptomatic degenerative rotator cuff tears. J Bone Joint Surg Am. 2015;97(2):89–98. doi: 10.2106/JBJS.N.00099. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Keener JD, Hsu JE, Steger-May K, Teefey SA, Chamberlain AM, Yamaguchi K. Patterns of tear progression for asymptomatic degenerative rotator cuff tears. J Shoulder Elb Surg. 2015;24(12):1845–1851. doi: 10.1016/j.jse.2015.08.038. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Namdari S, Donegan RP, Dahiya N, Galatz LM, Yamaguchi K, Keener JD. Characteristics of small to medium-sized rotator cuff tears with and without disruption of the anterior supraspinatus tendon. J Shoulder Elb Surg. 2014;23(1):20–27. doi: 10.1016/j.jse.2013.05.015. [DOI] [PubMed] [Google Scholar]
- 17.Keener JD, Skelley NW, Stobbs-Cucchi G, Steger-May K, Chamberlain AM, Aleem AW, Brophy RH. Shoulder activity level and progression of degenerative cuff disease. J Shoulder Elb Surg. 2017;26(9):1500–1507. doi: 10.1016/j.jse.2017.05.023. [DOI] [PubMed] [Google Scholar]
- 18.Dunn WR, Kuhn JE, Sanders R, An Q, Baumgarten KM, Bishop JY, Brophy RH, Carey JL, Holloway GB, Jones GL, Ma CB, Marx RG, McCarty EC, Poddar SK, Smith MV, Spencer EE, Vidal AF, Wolf BR, Wright RW. Symptoms of pain do not correlate with rotator cuff tear severity: a cross-sectional study of 393 patients with a symptomatic atraumatic full-thickness rotator cuff tear. J Bone Joint Surg Am. 2014;96(10):793–800. doi: 10.2106/JBJS.L.01304. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Maman E, Harris C, White L, Tomlinson G, Shashank M, Boynton E. Outcome of nonoperative treatment of symptomatic rotator cuff tears monitored by magnetic resonance imaging. J Bone Joint Surg Am. 2009;91(8):1898–1906. doi: 10.2106/JBJS.G.01335. [DOI] [PubMed] [Google Scholar]
- 20.Mall NA, Kim HM, Keener JD, Steger-May K, Teefey SA, Middleton WD, Stobbs G, Yamaguchi K. Symptomatic progression of asymptomatic rotator cuff tears: a prospective study of clinical and sonographic variables. J Bone Joint Surg Am. 2010;92(16):2623–2633. doi: 10.2106/JBJS.I.00506. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Safran O, Schroeder J, Bloom R, Weil Y, Milgrom C. Natural history of nonoperatively treated symptomatic rotator cuff tears in patients 60 years old or younger. Am J Sports Med. 2011;39(4):710–714. doi: 10.1177/0363546510393944. [DOI] [PubMed] [Google Scholar]
- 22.Fucentese SF, von Roll AL, Pfirrmann CWA, Gerber C, Jost B. Evolution of nonoperatively treated symptomatic isolated full-thickness supraspinatus tears. J Bone Joint Surg Am. 2012;94(9):801–808. doi: 10.2106/JBJS.I.01286. [DOI] [PubMed] [Google Scholar]
- 23.Moosmayer S, Tariq R, Stiris M, Smith H-J. The natural history of asymptomatic rotator cuff tears: a three-year follow-up of fifty cases. J Bone Joint Surg Am. 2013;95(14):1249–1255. doi: 10.2106/JBJS.L.00185. [DOI] [PubMed] [Google Scholar]
- 24.Hebert-Davies J, Teefey SA, Steger-May K, Chamberlain AM, Middleton W, Robinson K, Yamaguchi K, Keener JD. Progression of fatty muscle degeneration in atraumatic rotator cuff tears. J Bone Joint Surg Am. 2017;99(10):832–839. doi: 10.2106/JBJS.16.00030. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Chalmers PN, Salazar DH, Steger-May K, Chamberlain AM, Stobbs-Cucchi G, Yamaguchi K, Keener JD. Radiographic progression of arthritic changes in shoulders with degenerative rotator cuff tears. J Shoulder Elb Surg. 2016;25(11):1749–1755. doi: 10.1016/j.jse.2016.07.022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Varkey DT, Patterson BM, Creighton RA, Spang JT, Kamath GV. Initial medical management of rotator cuff tears: a demographic analysis of surgical and nonsurgical treatment in the United States Medicare population. J Shoulder Elb Surg. 2016;25(12):e378–e385. doi: 10.1016/j.jse.2016.05.001. [DOI] [PubMed] [Google Scholar]
- 27.Dunn WR, Kuhn JE, Sanders R, An Q, Baumgarten KM, Bishop JY, Brophy RH, Carey JL, Harrell F, Holloway BG, Jones GL, Ma CB, Marx RG, McCarty EC, Poddar SK, Smith MV, Spencer EE, Vidal AF, Wolf BR, Wright RW, MOON Shoulder Group 2013 Neer award: predictors of failure of nonoperative treatment of chronic, symptomatic, full-thickness rotator cuff tears. J Shoulder Elb Surg. 2016;25(8):1303–1311. doi: 10.1016/j.jse.2016.04.030. [DOI] [PubMed] [Google Scholar]
- 28.Moosmayer S, Gärtner AV, Tariq R. The natural course of nonoperatively treated rotator cuff tears: an 8.8-year follow-up of tear anatomy and clinical outcome in 49 patients. J Shoulder Elb Surg. 2017;26(4):627–634. doi: 10.1016/j.jse.2016.10.002. [DOI] [PubMed] [Google Scholar]
- 29.Kukkonen J, Joukainen A, Lehtinen J, Mattila KT, Tuominen EKJ, Kauko T, Äärimaa V. Treatment of nontraumatic rotator cuff tears: a randomized controlled trial with two years of clinical and imaging follow-up. J Bone Joint Surg Am. 2015;97(21):1729–1737. doi: 10.2106/JBJS.N.01051. [DOI] [PubMed] [Google Scholar]
- 30.Lambers Heerspink FO, van Raay JJAM, Koorevaar RCT, van Eerden PJM, Westerbeek RE, van’t Riet E, et al. Comparing surgical repair with conservative treatment for degenerative rotator cuff tears: a randomized controlled trial. J Shoulder Elb Surg. 2015;24(8):1274–1281. doi: 10.1016/j.jse.2015.05.040. [DOI] [PubMed] [Google Scholar]
- 31.Moosmayer S, Lund G, Seljom US, Haldorsen B, Svege IC, Hennig T, Pripp AH, Smith HJ. Tendon repair compared with physiotherapy in the treatment of rotator cuff tears: a randomized controlled study in 103 cases with a five-year follow-up. J Bone Joint Surg Am. 2014;96(18):1504–1514. doi: 10.2106/JBJS.M.01393. [DOI] [PubMed] [Google Scholar]
- 32.Park JS, Park HJ, Kim SH, Oh JH. Prognostic factors affecting rotator cuff healing after arthroscopic repair in small to medium-sized tears. Am J Sports Med. 2015;43(10):2386–2392. doi: 10.1177/0363546515594449. [DOI] [PubMed] [Google Scholar]
- 33.Tashjian RZ, Hung M, Burks RT, Greis PE. Influence of preoperative musculotendinous junction position on rotator cuff healing using single-row technique. Arthroscopy. 2013;29(11):1748–1754. doi: 10.1016/j.arthro.2013.08.014. [DOI] [PubMed] [Google Scholar]
- 34.Tan M, Lam PH, Le BTN, Murrell GAC. Trauma versus no trauma: an analysis of the effect of tear mechanism on tendon healing in 1300 consecutive patients after arthroscopic rotator cuff repair. J Shoulder Elb Surg. 2016;25(1):12–21. doi: 10.1016/j.jse.2015.06.023. [DOI] [PubMed] [Google Scholar]
- 35.Diebold G, Lam P, Walton J, Murrell GAC. Relationship between age and rotator cuff Retear: a study of 1,600 consecutive rotator cuff repairs. J Bone Joint Surg Am. 2017;99(14):1198–1205. doi: 10.2106/JBJS.16.00770. [DOI] [PubMed] [Google Scholar]
- 36.Robinson HA, Lam PH, Walton JR, Murrell GAC. The effect of rotator cuff repair on early overhead shoulder function: a study in 1600 consecutive rotator cuff repairs. J Shoulder Elb Surg. 2017;26(1):20–29. doi: 10.1016/j.jse.2016.05.022. [DOI] [PubMed] [Google Scholar]
- 37.Yeo DYT, Walton JR, Lam P, Murrell GAC. The relationship between intraoperative tear dimensions and postoperative pain in 1624 consecutive arthroscopic rotator cuff repairs. Am J Sports Med. 2017;45(4):788–793. doi: 10.1177/0363546516675168. [DOI] [PubMed] [Google Scholar]
- 38.Collin P, Kempf J-F, Molé D, Meyer N, Agout C, Saffarini M, Godenèche A, Société Française de Chirurgie Orthopédique et Traumatologique (SoFCOT) Ten-year multicenter clinical and MRI evaluation of isolated supraspinatus repairs. J Bone Joint Surg Am. 2017;99(16):1355–1364. doi: 10.2106/JBJS.16.01267. [DOI] [PubMed] [Google Scholar]
- 39.Hsu J, Keener JD. Natural history of rotator cuff disease and implications on management. Oper Tech Orthop. 2015;25(1):2–9. doi: 10.1053/j.oto.2014.11.006. [DOI] [PMC free article] [PubMed] [Google Scholar]