

Abstract
Study Objectives:
Even though the common diagnostic criteria (ICSD-3, DSM-5) acknowledge that nightmares do not only contain anxiety/fear (definition of the ICD-10) but also other emotions such as grief, disgust, and anger, the definition of a nightmare still focuses on threats to survival, security, or physical integrity. However, empirical studies on nightmare content in larger samples are scarce.
Methods:
The current study elicited 1,216 of the most recent nightmares including childhood nightmares of a population-based sample.
Results:
The findings show that nightmares encompass a diversity of different topics, being chased, physical aggression, including death/injury of close persons. Infrequent themes like being the aggressor and suicide are of special interest as they might be related to waking-life psychopathology.
Conclusions:
The variety of nightmare topics clearly indicate that current definitions of nightmare content are too narrow. Future studies should look into nightmare content of persons in whom nightmare disorder has been diagnosed.
Citation:
Schredl M, Göritz AS. Nightmare themes: an online study of most recent nightmares and childhood nightmares. J Clin Sleep Med. 2018;14(3):465–471.
Keywords: nightmare content, nightmare disorder, gender differences, psychopathology
BRIEF SUMMARY
Current Knowledge/Study Rationale: The definition of a nightmare given in diagnostic manuals (ICSD-3, DSM-5, ICD-10) focuses on threats to survival, security, or physical integrity. However, empirical studies on nightmare content in larger samples are scarce.
Study Impact: The findings of the current study clearly indicate that current definitions of nightmare content are too narrow (ie, death/injury of close persons is also an important nightmare theme). Infrequent themes such as being the aggressor and suicide are of special interest because they might be related to waking-life psychopathology.
INTRODUCTION
According to the International Classification of Sleep Disorders (ICSD-3)1 and the Diagnostic and Statistical Manual of Mental Disorders (DSM-5),2 nightmares are defined as “repeated occurrences of extended, extremely dysphoric, and well-remembered dreams that usually involve threats to survival, security, or physical integrity.” First, it should be noted that the types of negative emotions are not specified in these classifications, whereas the International Statistical Classification of Diseases and Related Health Problems (ICD-10)3 restricts nightmares to “dream experiences loaded with anxiety or fear” and uses the term “dream anxiety disorder” as a synonym. This change over time is based on empirical research that has shown that fear/panic is, in fact, the emotion occurring most often in nightmares but other emotions such as anger, disgust, grief, etc. might also be found in them.4–6 Second, the strict criterion that the dysphoric dream results in awakening has been loosened,1 even though research demonstrated that nightmares (with the awakening criterion) are more intense than bad dreams (dysphoric dreams without awakening).7,8 Despite these developments, the description of nightmare content (threats to survival, security, or physical integrity) still focuses on fear/panic and may not represent the diversity of nightmare themes. Interestingly, research regarding nightmare content is relatively scarce and often restricted to small clinical samples9,10 or student samples.4,11 The themes that came up in many studies4,9–16 are the following: being chased, threat of physical harm, injury and death of others, interpersonal conflicts, falling, failure, witnessing horror or violence, natural disaster, accidents, being late, and being paralyzed. These topics were also often found in typical dreams17–20 and recurrent dreams.21,22
As mentioned previously, large-scale studies on nightmare topics are scarce. Summaries of the two most comprehensive studies thus far follow. The top five themes in a representative German sample (n = 1,022) were falling, being chased, being paralyzed, being late (important event), and close persons disappear/die.23 These topics were chosen by 20% or more of the participants who experienced nightmares or bad dreams at least sometimes from a list of 23 themes. Analyzing 253 nightmares and 431 bad dreams collected via daily logs, Robert and Zadra24 obtained different results; the top-ranked themes were physical aggression, interpersonal conflicts, failure and helplessness, health-related concerns and death, and apprehension/worry, whereas falling dreams and being chased were less frequent. Despite the large sample size (n = 331) it should be noted that most of the sample consisted of students, even though some participants outside the university were recruited through media announcements. Interestingly, age and sex effects on the top five topics reported by Schredl were scarce: more females tended to report the topic of close persons disappear/die whereas no effects were found for falling dreams, being chased, and being paralyzed.23 Similarly, Robert and Zadra reported no sex effects for their five most common themes.24 The topic of being chased was much more common in childhood recurrent dreams compared to those of adults (41.5% versus 14.6%).21 Systematic research as to whether nightmare themes are related to nightmare frequency has not yet been carried out. To summarize, the research regarding nightmare topics indicate that nightmare content might not be exclusively limited to threats to survival, security, or physical integrity but also include others such as close persons disappear/die, interpersonal conflicts, and failure. The data base regarding nightmare topics in the general population is not solid, and questions regarding factors related to nightmare themes such as age, sex, or nightmare frequency are still unanswered.
The aim of the current study was to investigate the variety of nightmare themes in a sample drawn from the general population eliciting the most recent nightmare (including childhood nightmares). The applied classification was based on the study of Robert and Zadra.24 In addition, we looked for specific themes such as death/injury of others, falling, being chased, failing an examination, dreamer being the aggressor, and lucid dreams. The relationships between nightmare topics, age, sex, nightmare frequency, and nightmare occurrence (childhood versus adulthood) were studied in an exploratory fashion.
METHODS
Participants
Overall, 2,879 persons (1,784 female, 1,095 male) participated in the online study (www.wisopanel.net) carried out from March 23, 2011 to April 1, 2011. The mean age of the sample was 42.78 ± 12.24 years (range: 13 to 89 years).
One most recent nightmare was reported by 1,216 participants (860 female, 356 male) (ie, the percentage of reporting a nightmare was 42.24%). The mean age of this group was 41.98 ± 14.26 years (range: 18 to 83 years). The sample was quite evenly distributed along the following five age groups: younger than 30 years (n = 323), 30 to 39 years (n = 233), 40 to 49 years (n = 274), 50 to 59 years (n = 223), older than 60 years (n = 163). The females' mean age (39.88 ± 13.46 years) was lower than that of the males (47.04 ± 14.87 years, t = 7.9, P < .0001). The logistic regression of the report variable (Yes/ No) yielded a significant age effect (standardized estimate: .0453, χ2 = 3.9, P = .0478), a significant effect for sex (stan -dardized estimate: .1531, χ2 = 45.7, P < .0001), and a signifi-cant effect of nightmare frequency (standardized estimate: .2560, χ2 = 125.7, P < .0001). Older persons and persons with higher nightmare frequencies were more likely to report a most recent nightmare; 48.21% of the females reported a nightmare, whereas 32.51% of the males did so.
Measurement Instrument
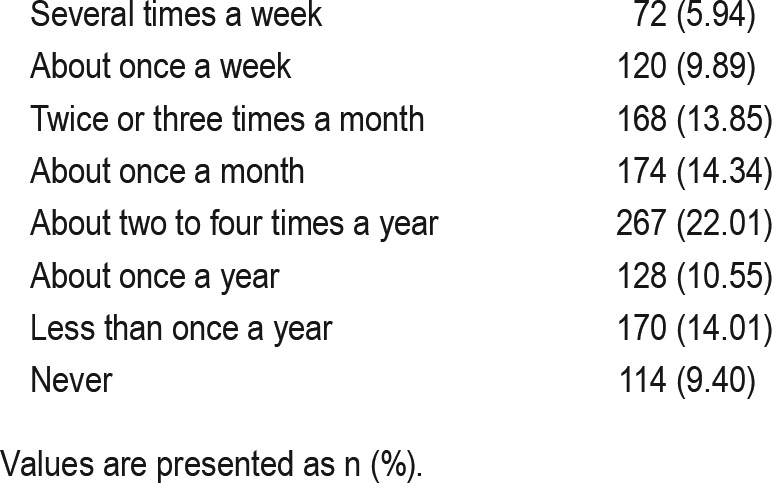
To assess nightmare frequency, an eight-point rating scale was presented (“How often do you experience nightmares?” 0: never, 1: less than once a year, 2: about once a year, 3: about 2 to 4 times a year, 4: about once a month, 5: about 2 to 3 times a month, 6: about once a week, 7: several times a week). Retest reliability of the nightmare frequency scale was high25: r = .75 (4 weeks retest interval).
Before reporting their most recent nightmares, the participants were asked to specify when the nightmare occurred; four categories were presented: during the last few weeks, during the last year, longer ago but during adulthood, or during childhood/adolescence. After the sentence: “Please report the most recent nightmare that you can remember, independently of whether it occurred last night, last week, last month or during childhood” the instructions for eliciting the most recent dreams26 were presented:
Please describe the dream exactly and as fully as you remember it. Your report should contain, whenever possible: a description of the setting of the dream, whether it was familiar to you or not; a description of the people, their age, sex, and relationship to you; and any animals that appeared in the dream. If possible, describe your feelings during the dream and whether it was pleasant or unpleasant. Be sure to tell exactly what happened during the dream to you and the other characters.
Classifying Dream Content
The classification of the nightmare themes was based on the suggestions given by Robert and Zadra.24 Based on their experience and the studies using the Typical Dream Questionnaire,18 they formulated 12 thematic categories: being chased (dreamer being chased by another character but not physically attacked); physical aggression (threat or direct attack to one's physical integrity by another character, including sexual aggression, murder, being kidnapped or sequestered); interpersonal conflicts (conflict-based interaction between two characters involving hostility, opposition, insults, humiliation, rejection, infidelity, lying, etc.); environmental abnormality (bizarre or implausible events appearing in the dream's environment); evil presence (seeing or feeling the presence of or being possessed by an evil force, including monsters, aliens, vampires, spirits, creatures, ghosts, etc.); accidents (the dreamer or another character is involved in an accident, including vehicle accidents, drowning, slipping, falling, etc.); disaster/calamity (plausible events ranging from relatively small-scale anomalies such as a fire or flood in one's house or neighborhood to large-scale disasters such as earthquakes, war, the end of the world, etc.); failure or helplessness (difficulty or incapacity of the dreamer to attain a goal, including being late, lost, unable to talk, losing or forgetting something, and making mistakes); insects/vermin (presence of or an infestation, bites or stings from insects, rats, snakes, etc.); health-related concerns and death (presence of physical illness, disease, health-related concerns, or death of a character or of the dreamer); apprehension/worry (dreamer is afraid or worried about someone or something, without an objective threat being present); and others (includes idiosyncratic as well as infrequent themes such as being naked, being self-critical, being in an insalubrious environment, and being unable to find/embarrassed to use a toilet). Based on previous studies,23,27 we were also interested in the following topics: falling dreams (subcategory of accidents); examination dreams (subcategory of failure or helplessness); sexual aggression (subcategory of physical aggression); lucidity (prelucid [thinking about whether it is a dream or not], lucid but not able to influence the course of action, lucid and, thus, able to awaken, and lucid with having an effect on actions and reactions during the dream); type of persecutor in dreams of being chased (male human, female human, humans of unknown sex, animals, creatures/things, and not specified); dreamer as aggressor as the main topic of the nightmare (eg, killing someone not in self-defense); suicide mentioned in the nightmare; and death/injury/serious threat to other dream characters that strongly concerns the dreamer (ie, is a major part of the nightmarish quality of the dream action [eg, death of close relatives, threat to one's children]).
Procedure
The study was approved by the local ethics committee. The link for the study was posted on an online panel: www.wiso-panel.net. Within this panel and after being informed about the purpose of the panel, persons with an interest in online studies and with heterogenic demographic backgrounds could register. For this study the participants could receive one euro if requested. The nightmare reports were edited in order to exclude all information not related to the dream experience itself and then classified along the aforementioned suggestions. A second independent judge classified 94 nightmares reports regarding the 12 themes.
Statistical procedures were carried out with the Statistical Analysis System software package version 9.4 for Windows (Cary, North Carolina, United States). Ordinal regressions (cumulative logit analyses) were used for analyzing the effects of different predictors on dream variables. For word count (logarithmic transformation), linear regression analyses have been computed.
RESULTS
Nightmare Frequency, Nightmare Length, and Nightmare Occurrence
Approximately 16% of the sample reported a nightmare frequency of one or more nightmares per week (see Table 1); most of the participants, however, were reporting occasional nightmares.
Table 1.
Nightmare frequency (n = 1,213).
Mean word count of the 1,216 nightmare reports was 60.06 ± 85.53 words with a large range from one word to 985 words. As the distribution of word count was skewed to the left, a logarithmic transformation (base 10) was applied. The mean log word count was 1.56 ± 0.45 (range: 0 to 2.99). The regression analyses of the transformed word count showed a significant effect of age (standardized estimate: −.1071, t = −3.7, P = .0002), a significant sex effect (standardized estimate: .1597, t = 5.6, P < .0001), and a significant effect of nightmare frequency (standardized estimate: .0736, t = 2.6, P = .0022). Older persons tend to report shorter nightmares, whereas persons with more frequent nightmares tended to report longer dreams. In addition, females reported longer dreams than males (67.66 ± 85.53 words versus 41.72 ± 45.77 words).
The occurrence of the most recent nightmare during the last few weeks was reported by 544 participants, during the last year (n = 234), longer ago but during adulthood (n = 237), and during childhood/adolescence (n = 189). The logistic regres -sion did not indicate either an age effect (standardized estimate: .0209, χ2 = 0.4, P = .5339) or a sex effect (standardized estimate: .0088, χ2 = 0.1, P = .7890) for nightmare occurrences, solely nightmare frequency was associated with this variable (standardized estimate: .9214, χ2 = 444.9, P < .0001). Persons with frequent nightmares were more likely to report a more recent nightmare.
Nightmare Topics
The exact agreement for classifying nightmare topics between the two raters was 76.5% (Cohen kappa = .53). Most of the nightmares (n = 1,076) contained only one topic, 137 nightmares two topics, and 3 nightmares three topics. The distribution for the total sample is depicted in Table 2. The most frequent topics are failure/helplessness, physical aggression, accidents, being chased, and health-related concerns and death. Nightmares including insects/vermin and environmental abnormality were quite rare. Comparing the current findings to Robert and Zadra24 including nightmares and bad dreams, the most striking differences are the following: physical aggression and interpersonal conflicts are less frequent in the current sample whereas accidents and being chased are more frequent (see Table 2). The distribution for the participants with frequent nightmares is relatively similar to the distribution of the total sample with the exception of more nightmares with interpersonal conflict and less often nightmares including accidents (see section on factors affecting nightmare themes).
Table 2.
Nightmare themes.

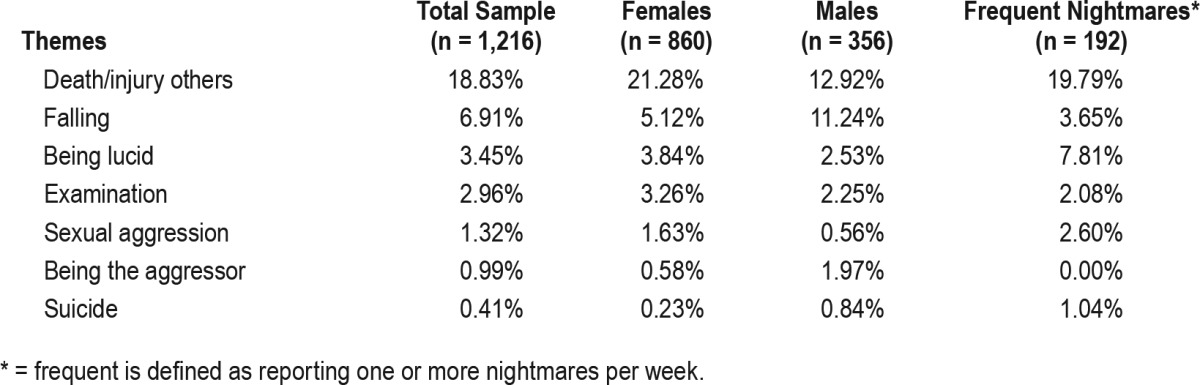
Table 3 indicates that death/injury/threats to others are fairly often a topic in nightmares and these nightmares often included family members (children, parents, or siblings); some of the nightmares also included pet animals. Falling dreams were fairly prominent compared to the figure of 1.5% reported by Robert and Zadra.24 The awareness of dreaming was present in 39 dreams; 3 dreams were prelucid (ie, the dreamer was thinking about whether this might be a dream or not but came to the conclusion that it was not a dream). In most of the lucid dreams (n = 20), the dreamer described that she or he still experienced fear or another negative emotion and was not able to change the dream action. Nine lucid dreamers reported that they applied their lucidity to deliberately wake themselves up, and in only 10 lucid dreams, the awareness of being lucid reduced anxiety and/or resulted in changing the course of the dream. Examinations (subtopic of failure/helplessness) was a topic in about 3% of the nightmares. In 12 nightmares, the dream ego committed an aggressive act (mostly murder) without being threatened (ie, not in self-defense) and the negative emotion was often remorse but sometimes fear of being found out. In five nightmares, the prominent topic was suicide, the dreamer killed himself twice, once the dreamer was on the edge of committing suicide, and two nightmares included the suicide of a parent (father, mother). Again, the distribution of the themes for the participants with frequent nightmare is roughly comparable with the distribution of the total sample.
Table 3.
Specific nightmare themes.
Perpetrators in Nightmares of Being Chased
If the dream ego was chased, the aggressor was classified if possible (see Table 4). If the sex of the human aggressor was known, 91.67% were male (44 out of 48). The percentages of the three categories humans, animals, and creatures/things— excluding the 44 cases with no information about the aggressor—were as follows: 59.52% (humans), 19.05% (animals), and 21.43% (creatures/things). The last category included monsters, ghosts, and devils and also objects such as a giant sphere chasing the dreamer.
Table 4.
Perpetrators in nightmares of being chased (n = 126).

Factors Affecting Nightmare Themes
In an exploratory fashion, the effects of age, sex, nightmare frequency, and nightmare occurrence (adulthood versus childhood) as independent variables on each of the nightmare themes (present or not present in the most recent nightmare) were studied by means of logistic regression analysis including all variables simultaneously. The logarithmic transformation of word count was also introduced to control for report length. Because 15 variables (all themes of Table 2, and additionally the themes of falling, examination, and death/injury of others) were studied, the number of statistical tests amounted to 60. Of those 60 tests, the results of 13 have been significant. Older persons were more likely to report dream themes of failure/ helplessness and less likely to report examination dreams. Females more often reported health-related concerns and death nightmares and nightmares including death/injury of others, whereas males more often reported falling dreams. Participants reporting nightmares more often had more nightmares including interpersonal conflict themes and less often nightmares with accidents. Childhood nightmares more often included being chased, evil presence, and falling, whereas the nightmares that occurred in adulthood more often included interpersonal conflicts and failure/helplessness. Due to small cell sizes, the sex differences for sexual aggression and being aggressor were tested with chi-square tests. Females reported marginally more nightmares with sexual aggression (χ2 = 2.2, P = .0689), whereas males reported more dreams of being the aggressor (χ2 = 4.9, P = .0131). No significant sex difference was found for suicide themes.
DISCUSSION
The current findings show that nightmares encompass a diversity of different topics, starting from classic threat dreams (being chased, physical aggression, or falling) to dreams of interpersonal conflicts or death/injury of close persons. Infrequent themes such as being the aggressor and suicide are of special interest because they might be related to waking-life psychopathology.
Before discussing the results in detail, several methodological issues have to be considered. The current sample consisted of most recent nightmares (ie, retrospectively remembered dreams). Robert and Zadra24 pointed out that this might cause a bias in the direction of more dramatic and intense nightmares compared to nightmares elicited with daily logs; the considerably larger number of falling dreams (extremely dramatic) in this sample compared to the figure obtained by Robert and Zadra24 would support this claim. However, it must be assumed that the selection bias will be larger if the study is more time-consuming by keeping a daily log for 2 to 5 weeks and recording dreams every morning (ie, only highly motivated persons with an interest in dreaming are likely to participate in diary studies). The sample of Robert and Zadra,24 for example, consisted of undergraduate students and persons recruited by media announcement for participating in a dream study. However, it should be noted that the advertisement did not address persons with nightmare complaints (eg, Hearne10) but persons with interest in dreams; this is also the case for the current study, which is clearly supported by the large variation regarding nightmare frequency. Also, the age range of the current sample is larger compared to Robert and Zadra24 (ie, the current findings complement those of their diary study). We found a significant sex effect on reporting a nightmare (while controlling for nightmare frequency), with females being more likely to report a most recent nightmare than males, a finding that has been reported for most recent dreams28 and for most recent bad dreams.27 Therefore, dream themes were also depicted for each sex separately, and sex was introduced in the exploratory regression analyses. It was expected that nightmare frequency is related to reporting a most recent nightmare but—as already mentioned—the participants providing nightmare reports still show a large variability of their nightmare frequency. Despite the wide age range of the sample, it should be noted that the sample is not representative; the persons of the panel are interested in participating in surveys of a large variety of topics (not sleep or dream focused). For these participants, unfortunately no data regarding mental health, physical health, and sleep are available. The word counts of the most recent nightmares vary considerably, from very brief reports such as “car accident” to very long dream reports. For dream content analyses using sophisticated coding systems such as the Hall and Van de Castle scales,29 typically dream reports between 50 and 300 words are included.26 If looking on thematic themes of dreams briefer dream reports can be included30; in the current study all nightmare reports could be classified. Cohen kappa is of moderate size,31 indicating that the definitions of the categories might be improvable. The percentage of correct matches is, however, comparable to other rating scales with similar complexity.29
The current study did not include any specific definition for nightmares; so it might be that nightmare reports of the current study might refer to other phenomena. The ICSD-31 is not reinforcing the awakening criterion for nightmares in particular:
Nightmare disorder is characterized by recurrent, highly dysphoric dreams, which are disturbing mental experiences that generally occur during REM sleep and that often result in awaking. (p. 258)
The distinction between nightmares (with awakening) and distressing or bad dreams (without awaking) might not be as important as the distressing nature of the dream content. So, it would be most interesting to study nightmare content in patients with a clinically diagnosed nightmare disorder. The high number of falling dreams (see also Schredl23) might point to a confusion of nightmares with hypnic jerks (also called “sleep starts”). Usually sleep starts include images of falling but are not accompanied by intense anxiety,32 but it would be interesting to study whether a definition for nightmares specifically excluding hypnic jerks at sleep onset would result in a smaller percentage of falling dreams.
The most often occurring themes (failure and helplessness, physical aggression, accidents, being chased, health-related concerns and death, interpersonal conflicts, and apprehension/ worry) matched the results of the Robert and Zadra24 study, with a shift to more dramatic themes (accidents and being chased). Less dramatic themes such as interpersonal conflicts have been reported less often—probably due to the methodological difference (most recent nightmares versus diary recorded nightmares). Based on the high prevalence of failure and helplessness topics and nightmares including death/injury of others, it might be advisable to adapt the nightmare definitions of the ICSD-31 and the DSM-52 that focus only on nightmares that include threats to the dreamer.
The distribution of nightmare themes in the current study are based on a sample of persons with varying nightmare frequency; from a clinical viewpoint, it would be very interesting to study patients with nightmare disorders (ie, those persons with clinically significant distress or impairment in social, occupational, or other important areas of functioning).1 The results regarding the participants with frequent nightmares (one or more nightmares per week; defined as nightmare disorder with moderate severity according to the DSM-5) might suggest that the nightmare topics in patients with nightmare disorder might be similar. Interestingly, nightmare frequency was related to the interpersonal conflicts in nightmares (ie, persons with a higher nightmare frequency dreamed more often about social topics). In accordance with the continuity hypothesis of dreaming,33 this could be due to problems in social functioning during the daytime. Because content analytic studies have not yet been carried out in patients with a formal diagnosis of nightmare disorder, it would be very interesting to study whether specific nightmare topics are related to the distress associated with this disorder.
The current study did not elicit any information about possible traumatic experiences that may have occurred in the lives of the participants. In two dream reports there was a link to previous events that were possibly traumatic (robbery and imprisonment). Previous research34,35 has shown that not all dreams after trauma are replicative (repetitions of the trauma), but dreams can also be related just by the basic emotion to the trauma. The rare occurrence of replicate dreams in the current sample does not rule out that some nightmares might be trauma related. In future studies, the history regarding trauma should be elicited in addition to nightmare content, in order to study whether nonreplicative nightmares in persons with trauma resemble those of idiopathic nightmares.
The most pronounced sex difference was that females more often reported nightmares involving death/injury of a signifi-cant other, a finding that is supported by sex differences regarding relationship closeness in waking.36 Males more often reported falling dreams, a finding that warrants further clarification. The finding that older persons more often reported nightmares of failure and younger persons more often examination dreams (this was also reported by Schredl23) fit with the continuity hypothesis of dreaming33 as younger persons do undergo more examinations in their waking life and older persons might have issues with decreasing capabilities.
Confirming the findings of Zadra,21 we found dreams of being chased more often in childhood nightmares compared to those occurring in adulthood. This preponderance in childhood nightmares was also found for falling dreams and evil presence themes, whereas the topics of failure/helplessness and interpersonal conflicts were more often found in adult nightmares. Again, it would be very interesting to study children in whom nightmare disorders have been diagnosed in order to compare their dreams with nightmares in adults.
A small percentage of nightmares (about 1%) were characterized by the dreamer as the aggressor and not the victim. This is of interest because two studies37,38 showed that extreme aggressive acts committed in the dream are related to waking life aggressiveness of the dreamer. The sex difference with males being more often aggressive in their dreams is supported by previous findings39 and also waking-life differences in aggression.40 Interestingly, this also corresponds with the sex difference in dream aggressors (ie, if the sex of a human aggressor in dreams of being chased was mentioned it was predominantly a male character, a finding previously reported by Schredl and Pallmer27). This reflects the fact that violent crimes are most often committed by males.41
Correlations studies42,43 found a significant correlation between lucid dreaming frequency and nightmare frequency, which can be explained by bizarre aspects of nightmares triggering lucidity but also seems contradictory because lucid dreaming is an effective coping strategy for nightmares.44,45 The current findings helped clarify this discrepancy because most nightmares including lucidity did not help reduce the fear while dreaming (no effect at all or just trying to waking up). The concept that the dreamer can influence the course of action during lucid dreams should be promoted if this method is to be used in treating nightmares as a second-choice treatment to the well-established imagery rehearsal therapy.46
Last, several studies47–49 indicated that nightmares might be an independent risk factor for committing suicide. Whereas Perlis et al.50 suggested that the time of night plays an important role (ie, being more vulnerable to suicide in the nighttime hours), the current findings indicate that sometimes nightmares themselves might trigger suicidal behavior because they included this possibility explicitly. This seems plausible as nightmares can also trigger panic attacks.51 Within the clinical context, it should be explored as to whether persons with suicide topics in their nightmares also show suicidal ideation during waking.
To summarize, the themes of nightmares are manifold, including themes such as failure and death/injury to significant others and, thus, the current definitions of nightmare content in the ICSD-3 and DSM-5 should be expanded. Future research should focus on persons with clinically diagnosed nightmare disorder and the relationship between nightmare content and waking-life distress and impairment in these patients. Retrospective studies should be complemented with diary studies, especially in those who have nightmares and are highly stressed. In addition, it would be very interesting to validate the severity criteria of the DSM-5 based on frequency (eg, moderate severity as one or more nightmares per week but less than nightly). That is, how close is the relationship between nightmare frequency and clinically significant distress and impairment?
DISCLOSURE STATEMENT
Work for this study was performed at Central Institute of Mental Health, Mannheim, Germany. Both authors have seen and approved the manuscript. The authors report no conflicts of interest.
ABBREVIATIONS
- DSM
Diagnostic and Statistical Manual of Mental Disorders
- ICD
International Statistical Classification of Diseases and Related Health Problems
- ICSD
International Classification of Sleep Disorders
REFERENCES
- 1.American Academy of Sleep Medicine. International Classification of Sleep Disorders. Darien, IL: American Academy of Sleep Medicine; 2014. [Google Scholar]
- 2.American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. Washington, DC: American Psychiatric Association; 2013. [Google Scholar]
- 3.World Health Organization. The ICD-10 Classification of Mental and Behavioural Disorders: Clinical Descriptions and Diagnostic Guidelines. Geneva, Switzerland: World Health Organization; 1992. [Google Scholar]
- 4.Dunn KK, Barrett D. Characteristics of nightmare subjects and their nightmares. Psychiatr J Univ Ott. 1988;13(2):91–93. [PubMed] [Google Scholar]
- 5.Zadra AL, Pilon M, Donderi DC. Variety and intensity of emotions in nightmares and bad dreams. J Nerv Ment Dis. 2006;194(4):249–254. doi: 10.1097/01.nmd.0000207359.46223.dc. [DOI] [PubMed] [Google Scholar]
- 6.Rose MW, Perlis ML, Kaszniak AW. Self-reported dream emotion: nightmares and vivid dreams. Sleep Res. 1992;21:132. [Google Scholar]
- 7.Fireman GD, Levin R, Pope AW. Narrative qualities of bad dreams and nightmares. Dreaming. 2014;24:112–124. [Google Scholar]
- 8.Zadra AL, Donderi DC. Nightmares and bad dreams: their prevalence and relationship to well-being. J Abnorm Psychol. 2000;109(2):273–281. [PubMed] [Google Scholar]
- 9.Kales A, Soldatos CR, Caldwell AB, et al. Nightmares: clinical characteristics and personality pattern. Am J Psychiatry. 1980;137(10):1197–1201. doi: 10.1176/ajp.137.10.1197. [DOI] [PubMed] [Google Scholar]
- 10.Hearne KM. A questionnaire and personality study of nightmare sufferers. Journal of Mental Imagery. 1991;15(3-4):55–64. [Google Scholar]
- 11.Cellucci AJ, Lawrence PS. The efficacy of systematic desensitization in recurring nightmares. J Behav Ther Exp Psychiatry. 1978;9:109–114. [Google Scholar]
- 12.Gauchat A, Séguin JR, McSween-Cadieux E, Zadra AL. The content of recurrent dreams in young adolescents. Conscious Cogn. 2015;37:103–111. doi: 10.1016/j.concog.2015.08.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Taub JM, Kramer M, Arand D, Jacobs GA. Nightmare dreams and nightmare confabulations. Compr Psychiatry. 1978;19(3):285–291. doi: 10.1016/0010-440x(78)90049-4. [DOI] [PubMed] [Google Scholar]
- 14.Feldman MJ, Hyman E. Content analysis of nightmare reports. Psychophysiology. 1968;5:221. [Google Scholar]
- 15.Cernovsky ZZ. Content of waking life events and of nightmare themes. Percept Mot Skills. 1984;58(3):899–902. doi: 10.2466/pms.1984.58.3.899. [DOI] [PubMed] [Google Scholar]
- 16.Zadra AL, Duval M, Begin E, Pilon M. Content analysis of nightmares [abstract] Sleep. 2004;27:A64. [Google Scholar]
- 17.Yin F, Shen H, He Y, Wei Y, Cao W. Typical dreams of “being chased”: a cross-cultural comparison between Tibetan and Han Chinese dreamers. Dreaming. 2013;23:64–77. [Google Scholar]
- 18.Nielsen TA, Zadra AL, Simard V, et al. The typical dreams of Canadian university students. Dreaming. 2003;13:211–235. [Google Scholar]
- 19.Yu CK. Typical dreams experienced by Chinese people. Dreaming. 2008;18:1–10. [Google Scholar]
- 20.Schredl M, Ciric P, Götz S, Wittmann L. Typical dreams: stability and gender differences. J Psychol. 2004;138(6):485–494. doi: 10.3200/JRLP.138.6.485-494. [DOI] [PubMed] [Google Scholar]
- 21.Zadra AL. Recurrent Dreams: Their Relationship to Life Events. In: Barrett D, editor. Trauma and Dreams. Cambridge, MA: Harvard University Press; 1996. pp. 231–247. [Google Scholar]
- 22.Zadra AL, Desjardins S, Marcotte E. Evolutionary function of dreams: a test of the threat simulation theory in recurrent dreams. Compr Psychiatry. 2006;15(2):450–463. doi: 10.1016/j.concog.2005.02.002. [DOI] [PubMed] [Google Scholar]
- 23.Schredl M. Nightmare frequency and nightmare topics in a representative German sample. Eur Arch Psychiatry Clin Neurosci. 2010;260(8):565–570. doi: 10.1007/s00406-010-0112-3. [DOI] [PubMed] [Google Scholar]
- 24.Robert G, Zadra AL. Thematic and content analysis of idiopathic nightmares and bad dreams. Sleep. 2014;37(2):409–417. doi: 10.5665/sleep.3426. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Stumbrys T, Erlacher D, Schredl M. Reliability and stability of lucid dream and nightmare frequency scales. Int J Dream Res. 2013;6:123–126. [Google Scholar]
- 26.Domhoff GW. Finding Meaning In Dreams: A Quantitative Approach. New York, NY: Plenum Press; 1996. [Google Scholar]
- 27.Schredl M, Pallmer R. Geschlechtsunterschiede in Angstträumen von SchülerInnen. Prax Kinderpsychol Kinderpsychiatr. 1998;47:463–476. [PubMed] [Google Scholar]
- 28.Winget C, Kramer M, Whitman RM. Dreams and demography. Can Psychiatr Assoc J. 1972;17(2) Suppl 2:SS203. doi: 10.1177/07067437720176s232. [DOI] [PubMed] [Google Scholar]
- 29.Hall CS, Van de Castle RL. The Content Analysis of Dreams. New York, NY: Appleton-Century-Crofts; 1966. [Google Scholar]
- 30.Schredl M. Dream content analysis: basic principles. Int J Dream Res. 2010;3:65–73. [Google Scholar]
- 31.Altman DG. Practical Statistics for Medical Research. London, UK: Chapman and Hall; 2016. [Google Scholar]
- 32.Salas RE, Gulyani S, Kwan AB, Gamaldo CE. Sleep-Related Movement Disorders and Their Unique Motor Manifestations. In: Kryger M, Roth T, Dement WC, editors. Principles and Practice of Sleep Medicine. 6th ed. Philadelphia, PA: Elsevier; 2016. pp. 1020–1029. [Google Scholar]
- 33.Schredl M. Continuity between waking and dreaming: a proposal for a mathematical model. Sleep Hypn. 2003;5:38–52. [Google Scholar]
- 34.Wittmann L, Schredl M, Kramer M. The role of dreaming in posttraumatic stress disorder. Psychother Psychosom. 2007;76:25–39. doi: 10.1159/000096362. [DOI] [PubMed] [Google Scholar]
- 35.Duval M, Zadra AL. Frequency and content of dreams associated with trauma. Sleep Med Clin. 2010;5:249–260. [Google Scholar]
- 36.Marshall TC. Gender, Peer Relations, and Intimate Romantic Relationships. In: Chrisler JC, McCreary DR, editors. Handbook of Gender Research in Psychology. New York, NY: Springer; 2010. pp. 281–310. [Google Scholar]
- 37.Renvert M. Wenn man im Traum zum Täter wird [diploma thesis] University of Düsseldorf; 2007. [Google Scholar]
- 38.Schredl M, Mathes J. Are dreams of killing someone related to waking-life aggression? Dreaming. 2014;24:176–181. [Google Scholar]
- 39.Schredl M. Gender Differences in Dreaming. In: Barrett D, McNamara P, editors. Praeger Perspectives. The New Science of Dreaming: Vol. 2. Content, Recall, and Personality Correlates. Westport, CT: Praeger/Greenwood; 2007. pp. 29–47. [Google Scholar]
- 40.Lansford JE, Skinner AT, Sorbring E, et al. Boys' and girls' relational and physical aggression in nine countries. Aggress Behav. 2012;38(4):298–308. doi: 10.1002/ab.21433. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Broidy L, Agnew R. Gender and crime: a general strain theory perspective. J Res Crime Delinq. 1997;34:275–306. [Google Scholar]
- 42.Schredl M, Erlacher D. Lucid dreaming frequency and personality. Pers Individ Dif. 2004;37:1463–1473. [Google Scholar]
- 43.Stepansky R, Holzinger B, Schmeiser-Rieder A, Saletu B, Kunze M, Zeitlhofer J. Austrian dream behavior: results of a representative population survey. Dreaming. 1998;8:23–30. [Google Scholar]
- 44.Spoormaker VI, Van den Bout J. Lucid dreaming treatment for nightmares: a pilot study. Psychother Psychosom. 2006;75(6):389–394. doi: 10.1159/000095446. [DOI] [PubMed] [Google Scholar]
- 45.Zadra AL, Pihl RO. Lucid dreaming as a treatment for recurrent nightmares. Psychother Psychosom. 1997;66(1):50–55. doi: 10.1159/000289106. [DOI] [PubMed] [Google Scholar]
- 46.Krakow B, Zadra AL. Imagery rehearsal therapy: principles and practice. Sleep Med Clinics. 2010;5:289–298. [Google Scholar]
- 47.Sjöström N, Waern M, Hetta J. Nightmares and sleep disturbances in relation to suicidality in suicide attempters. Sleep. 2007;30(1):91–95. doi: 10.1093/sleep/30.1.91. [DOI] [PubMed] [Google Scholar]
- 48.Wong HK, Swinea JC, Winer S, Nadorff MR. The association between nightmares and suicide risk is cross-sectionally mediated by borderline symptoms [abstract] Sleep. 2014;37:A288. [Google Scholar]
- 49.Tanskanen A, Tuomilehto J, Viinamäki H, Vartiainen E, Lehtonen J, Puska P. Nightmares as predictors of suicide. Sleep. 2001;24(7):844–847. [PubMed] [Google Scholar]
- 50.Perlis ML, Grandner MA, Chakravorty S, Bernert RA, Brown GK, Thase ME. Suicide and sleep: Is it a bad thing to be awake when reason sleeps? Sleep Med Rev. 2015;29:101–107. doi: 10.1016/j.smrv.2015.10.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Schredl M, Kronenberg G, Nonell P, Heuser I. Dream recall, nightmare frequency, and nocturnal panic attacks in patients with panic disorder: their relationship to nocturnal panic attacks. J Nerv Ment Dis. 2001;189:559–562. doi: 10.1097/00005053-200108000-00011. [DOI] [PubMed] [Google Scholar]