
Fig.1.
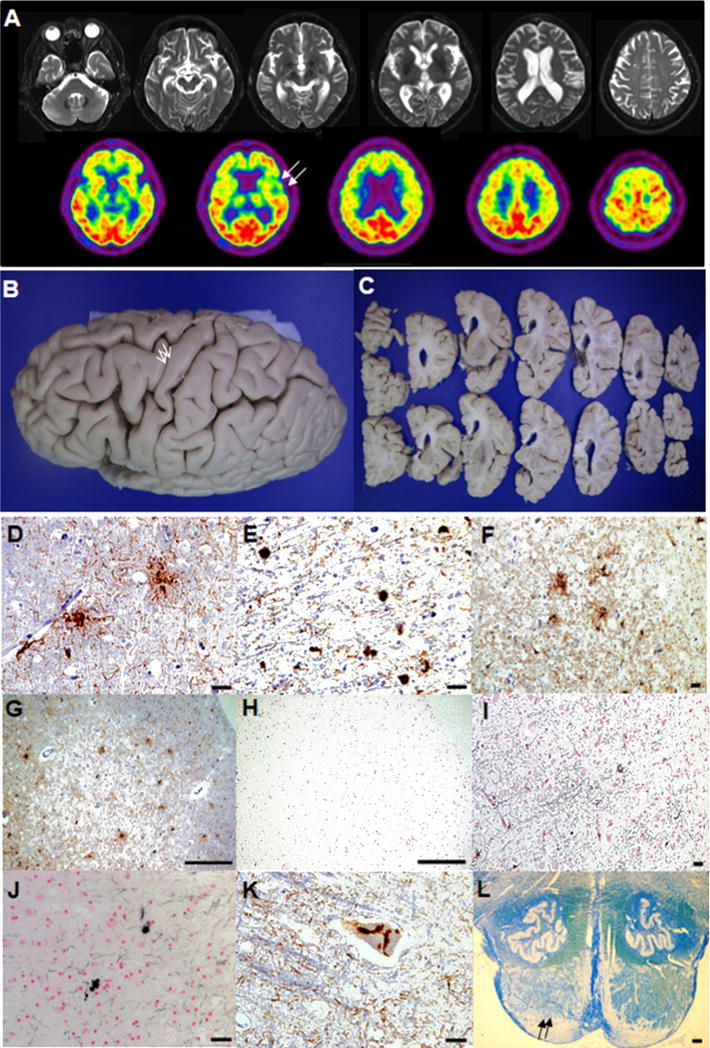
(A)Brain MRIs at age 78 demonstrated diffuse cortical atrophy, worse on the frontal than parietal with dilated ventricle (upper row). 18[F]-fluorodeoxyglucose (FDG)-PET showed glucose hypometabolism in bilateral frontotemporal area including severe glucose hypometabolism in the left frontal opercular area (lower row, arrows). (B)Widening of the superior and middle frontal sulci, and grossly preserved precentral cortex (arrows) were detected in the formalin-fixed left hemisphere. (C)The coronal sections of the left hemisphere displayed moderate atrophy in dorsolateral frontal and inferior frontal cortices with mildly dilated frontal horn and the lateral ventricle. (D)GAIs in the middle frontal cortex (CP-13, scale bar = 25 μm). (E)GOIs and coiled bodies in the subcortical white matter of superior frontal sulcus (CP-13, scale bar = 25 μm). (F)4R tau positive GAIs and threads in the precentral cortex (RD 4, scale bar = 250 μm). (G)Tau immunoreactive GAIs in the prefrontal cortex (CP-13, scale bar = 250 μm). (H, I)No evidence of Gallyas positive GAIs was detected in the same prefrontal cortex as (G) (Gallyas, scale bar = 250 μm) and the superior frontal sulcus (Gallyas, scale bar = 250 μm). (J)Gallyas positive GOIs and coiled bodies in the subcortical white matter of superior frontal sulcus (Gallyas, scale bar = 25 μm). (K)Tau immunoreactive neuronal cytoplasmic inclusions in Betz cell of precentral cortex (CP-13, scale bar = 25 μm). (L)Myelin pallor (arrows) was seen in the pyramid of the pontomedullary junction (Luxol Fast Blue stain, scale bar = 500 μm).