

Abstract
Background
Care of patients with trauma is not only limited to the sustained physical injuries but also requires addressing social issues, such as substance abuse and interpersonal violence, which are responsible for trauma-related recidivism. This study investigates whether there are age-related variations in these problematic social behaviors to analyze whether there is an age cut-off at which point adolescents should be screened for adult social behaviors.
Methods
Retrospective review of patients with trauma aged 12–21 admitted to an urban Level 1 adult and pediatric trauma center between February 2013 and April 2016. Demographics, mechanisms of injury, Injury Severity Score, outcomes, toxicology and social history evaluations were abstracted from the electronic medical record.
Results
756 patients were admitted during the 39-month period. Most patients were male (73.9%) without significant variation by age. The mechanisms of injury varied by age (p<0.001) with the incidence of sports and bicycle injuries decreasing and the incidence of motor vehicle/motorcycle crashes, assaults and gunshot injuries increasing with increasing patient age. In a logistic regression, risks of positive toxicology tests, injuries due to violence as well as overall use of drugs, tobacco and alcohol also significantly increased with age starting with the youngest age included in the study.
Conclusions
As pediatric trauma patients get older, they have increasing risks of social issues typically associated with adults. Our study underscores the need to evaluate and address these issues even in young adolescents.
Level of evidence
Level IV—epidemiological.
Keywords: recidivism, pediatric trauma, alcohol abuse, substance abuse, injury prevention
Background
Although often considered an acute and singular occurrence, trauma can unfortunately be a recurrent phenomenon for some patients. This trauma recidivism, defined as recurrent, separate incidences of traumatic injury, has been linked with certain social risk factors, including alcohol and substance abuse and interpersonal violence.1 2 In one systematic review, trauma recidivism was linked to alcohol use in as many as 41% of patients.3 In adult patients, brief in-hospital intervention programs have been demonstrated to reduce recurrent injuries due to both substance abuse and interpersonal violence.1 4 As a consequence of these data, the American College of Surgeons Committee on Trauma Verification Review process mandates that all Level I and Level II trauma centers have active screening and brief intervention programs.5
In the pediatric population, patients are screened less commonly for these high-risk adult behaviors despite recommendation from the Pediatric Trauma Society for alcohol screening in all patients 12 years or older.6 7 A Canadian study demonstrated that blood alcohol concentration was tested in only 30% of pediatric patients admitted after major trauma with 21% of those positive.8 A review of severely injured pediatric patients from the Illinois State trauma registry (1999–2009) demonstrated that only 40% were tested for alcohol and 37% for drugs.7
The data on the incidence of these high-risk behaviors in pediatric trauma populations are incomplete. Previous studies used toxicology tests at the time of the admission to measure the incidence of alcohol and substance abuse. Therefore, they may potentially underestimate the overall incidence as some patients may still use these substances, although not immediately prior to the trauma. In addition, prior studies have focused on severely injured patients rather than all admitted patients. In this study, we sought to further investigate the incidence of these high-risk social behaviors and establish an age cut-off at which point all adolescents should be screened. We hypothesized that there exists an age threshold at which there would be an increase in the incidence of these high-risk behaviors. We further hypothesized that this threshold would occur at the age of 14, the most common age of high school entry.
Methods
Yale New Haven Hospital is an urban, American College of Surgeons verified and state designated Level I regional resource trauma center and quaternary referral center for both adult and pediatric patients. Query of the Yale-New Haven Hospital’s trauma registry (TraumaBase; Clinical Data Management, Denver, CO) identified all patients aged 12–21 years admitted to the hospital between February 2013 and April 2016. The trauma registry and electronic medical record (EMR) (EPIC, Verona, WI) was then reviewed to abstract demographics, mechanisms of injury, Injury Severity Score (ISS), outcomes, and toxicology results. Alcohol and drug use were abstracted from both toxicology results and detailed EMR review to identify reported substance use in physician notes (history and physical notes, consult notes and tertiary trauma surveys) and social worker evaluations. Both the tertiary trauma survey and trauma social work evaluations used standardized template that included specific questions on alcohol and substance use. Any documented use of alcohol or drug in any of the notes was captured as a positive screen.
Statistical analysis
Statistical analysis was performed using IBM SPSS Statistics V.24 using ANOVA, χ2, linear and logistic regression as appropriate; statistical significance was assumed for p<0.05.
Results
Seven hundred and fifty-six patients who met the inclusion criteria were admitted during the 39-month period. Figure 1 shows the distribution of patients by age. Most were male (73.9%) without significant variation in gender across the age groups (Χ2 (9)=10.3, p=0.3). The mechanisms of injury did vary with age (Χ2 (117)=290, p<0.001) with the incidence of sports and bicycle injuries decreasing and the incidence of motor vehicle/motorcycle crashes, assaults and gunshot injuries increasing with increasing patient age (table 1). The median ISS was 5 (IQR=4–12) and slightly increased with age in a simple regression (R=0.123, p<0.001). Overall, 17% of the patients had ISS>15; there was no significant variation in the rate of severe injury across the age groups (R=0.153, p=0.08). Median length of stay was 2 days (IQR=1–4) and slightly increased with increasing age (R=0.164, p<0.01).
Figure 1.
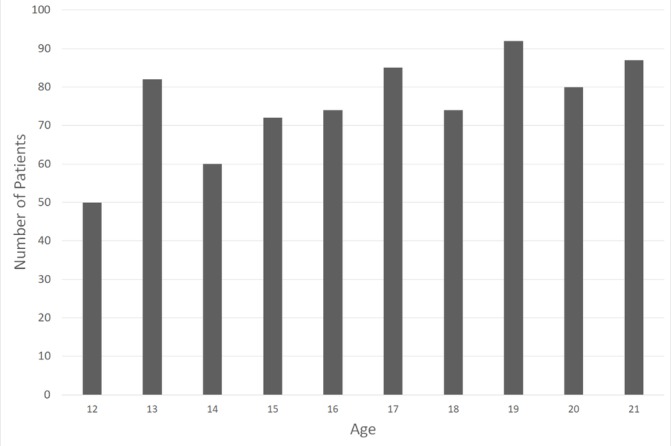
Distribution of patients by age group.
Table 1.
Mechanism of injury across ages
| Age | 12 (%) | 13 (%) | 14 (%) | 15 (%) | 16 (%) | 17 (%) | 18 (%) | 19 (%) | 20 (%) | 21 (%) | All ages (%) |
| Fall from standing | 12 | 4.9 | 13.3 | 6.9 | 6.8 | 5.9 | 6.8 | 4.3 | 2.5 | 8.0 | 6.7 |
| Fall from height | 6 | 3.7 | 10.0 | 6.9 | 8.1 | 8.2 | 8.1 | 7.6 | 3.8 | 5.7 | 6.7 |
| Assault | 0 | 1.2 | 0 | 5.6 | 1.4 | 8.2 | 5.4 | 9.8 | 8.8 | 6.9 | 5.2 |
| GSW | 0 | 3.7 | 1.7 | 5.6 | 10.8 | 9.4 | 12.2 | 14.1 | 15.0 | 9.2 | 8.7 |
| Stab | 0 | 0 | 0 | 0 | 1.4 | 0 | 2.7 | 3.3 | 1.3 | 5.7 | 1.6 |
| MVC passenger | 4 | 4.9 | 3.3 | 12.5 | 6.8 | 2.4 | 12.2 | 8.7 | 10.0 | 11.5 | 7.8 |
| MVC driver | 0 | 2.4 | 0 | 0 | 5.4 | 8.2 | 28.4 | 10.9 | 22.5 | 24.1 | 11.0 |
| MCC driver | 4 | 2.4 | 8.3 | 9.7 | 4.1 | 5.9 | 6.8 | 9.8 | 10.0 | 10.3 | 7.3 |
| MCC passenger | 0 | 2.4 | 1.7 | 0 | 0 | 0 | 0 | 1.1 | 0 | 0 | 0.5 |
| Bicycle | 22.0 | 14.6 | 18.3 | 9.7 | 4.1 | 2.4 | 1.4 | 1.1 | 2.5 | 1.1 | 6.7 |
| Pedestrian struck | 8.0 | 7.3 | 5.0 | 4.2 | 14.9 | 10.6 | 4.1 | 9.8 | 3.8 | 4.6 | 7.3 |
| Sports | 32.0 | 37.8 | 28.3 | 29.2 | 27.0 | 31.8 | 8.1 | 12.0 | 12.5 | 6.9 | 21.8 |
| Burn | 2.0 | 2.4 | 1.7 | 1.4 | 1.4 | 1.2 | 0 | 1.1 | 1.3 | 2.3 | 1.5 |
| Other | 10.0 | 12.2 | 8.3 | 8.3 | 8.1 | 5.9 | 4.1 | 6.5 | 6.3 | 3.4 | 7.1 |
GSW, gunshot wound; MVC, motor vehicle crash; MCC, motorcycle crash.
Alcohol was tested in 341 patients (45% of the study cohort) and was positive in 29.2% of those tested (table 2). Positive alcohol toxicology rates ranged from 0% at the age of 12 to 50% at the age of 21. Toxicology screens (cannabinoid, cocaine, phencyclidine, amphetamines) were sent in 356 patients (47% of the study cohort) and were positive for at least one substance in 32.9% of those tested. Cannabinoid was the most common substance used (21.6% positive of those tested). Opiate and benzodiazepine tests were not evaluated as available data could not differentiate between those administered by healthcare providers versus those self-administered by the patient.
Table 2.
Rates of high-risk behaviors by age
| Age | 12 | 13 | 14 | 15 | 16 | 17 | 18 | 19 | 20 | 21 | All ages | OR | P values |
| Positive alcohol toxicology, % (n-tested)* | 0 (3) | 8.3 (12) | 37.5 (8) | 11.1 (18) | 16.7 (36) | 14.0 (43) | 29.1 (55 | 30.4 (56) | 37.3 (51) | 50.0 (60) | 29.2 (342) | 1.34 | 0.001 |
| Positive drug toxicology, % (n-tested)* | 33.3 (3) | 0 (14) | 12.5 (8) | 38.9 (18) | 27.8 (36) | 34.0 (47) | 32.1 (56) | 32.8 (61) | 40.4 (52) | 37.7 (61) | 32.9 (356) | 1.13 | 0.02 |
| Injury due to interpersonal violence, % (N)† | 0 (50) | 4.9 (82) | 5.0 (60) | 9.7 (72) | 12.2 (74) | 16.5 (85) | 16.2 (74) | 27.2 (92) | 22.5 (80) | 20.7 (87) | 14.6 (756) | 1.27 | 0.001 |
| Tobacco use, % (N)† | 0 (50) | 1.2 (82) | 3.3 (60) | 5.6 (72) | 9.5 (74) | 16.5 (85) | 18.9 (74) | 25.0 (92) | 22.5 (80) | 19.5 (87) | 13.2 (756) | 1.34 | 0.001 |
| Overall substance use, % (N)† | 0 (50) | 2.4 (82) | 3.3 (60) | 6.9 (72) | 16.2 (74) | 25.9 (85) | 27.0 (74) | 34.8 (92) | 31.3 (80) | 26.4 (87) | 18.9 (756) | 1.35 | 0.001 |
| Overall alcohol use, % (N)† | 0 (50) | 3.7 (82) | 5.0 (60) | 6.9 (72) | 12.2 (74) | 24.7 (85) | 39.2 (74) | 41.3 (92) | 48.8 (80) | 57.5 (87) | 26.1 (756) | 1.58 | 0.001 |
*n-tested: number of patients who had alcohol or drug toxicology drawn in age group.
†N: number of patients in each age group.
Calculation of the incidence using only positive laboratory tests yielded a rate of 13.2% (100/756) for ethanol and 15.5% (117/756) for illicit substance use. However, after examining the electronic medical record for reported use in physician and social worker evaluations in addition to laboratory tests, the overall rates were higher (table 2). After combining laboratory and clinician detected use, 26.1% (197/756) were positive for alcohol and 18.9% (143/756) for drug use. In addition, 13.2% (100/756) of the cohort reported smoking cigarettes. Interpersonal violence, resulting in assault, firearm or stabbing injuries, was responsible for 14.6% (110/756) of the admissions and increased with age (p<0.001).
In a logistic regression, risks of positive toxicology tests, injuries due to violence as well as use of drugs, tobacco and alcohol in social history also significantly increased with age (table 2) starting with the youngest age group included in the study.
Discussion
The best management of traumatic injuries is to prevent them. Current literature has demonstrated that certain high-risk behaviors lead to trauma recidivism and that inpatient interventions targeting these behaviors can help decrease recurrent injuries.9 10 However, as healthcare resources are limited, it is important to understand the incidence of these behaviors and which patient populations should be targeted to maximize the opportunity for injury prevention. Our study demonstrates that these high-risk behaviors occur even in early adolescence. Furthermore, these data suggest that the evidence available in the current literature based on laboratory testing underestimates the actual incidence.
Pediatric patients with trauma represent a unique population as interventions to reduce these behaviors may have a lengthy impact and could potentially translate into substantial quality-adjusted life years saved not only from future traumatic injuries but also other medical problems that arise from alcohol and substance abuse. In 2006, The National Institute of Health estimated that approximately 5000 people under the age of 21 die each year as a result of alcohol including 1600 from homicide and 300 from suicide.11 The rate of lifetime dependency among individuals who start drinking before the age of 15 is four times higher (40 vs 10%) than those who start drinking as adults.12 Early onset of drug use is also a significant predictor of subsequent development of lifetime drug abuse and alcohol dependence.13 As alcohol is the third leading cause of preventable death in the USA (estimated 88 000 deaths per year), preventing the development of alcohol abuse early may have significant public health benefits.14
Brief interventions have been shown to reduce both trauma recidivism and subsequent use of both alcohol and illicit substances. In a study of adult patients with trauma in Spain who were positive for alcohol or drug use, the adjusted HR for trauma recidivism was 0.63 (95% CI 0.41 to 0.95) in the group who underwent a brief intervention compared with those that did not.4 The overall rate of trauma recidivism was, however, still higher in the patients positive for drug or alcohol compared with those who were negative. Furthermore, in a randomized controlled trial of underage drinkers (aged 14–20 years) in the emergency department, brief intervention was shown to reduce consumption at 3 months as well as the frequency of driving under influence and alcohol-related injury at 12 months.15
This study has limitations including its retrospective single-center nature. Yale New Haven Hospital is an academic urban safety net hospital. As one of only two Level I adult and pediatric trauma centers in the state of Connecticut (with a population of approximately 3.6 million), it serves a wide range of urban, suburban and rural populations. However, the incidence of the reported high-risk behaviors in our center may not be translatable to other communities. In addition, this study may be limited by selection bias as laboratory tests were ordered selectively rather than universally. Furthermore, some patients may have also falsely denied use during history taking and we did not examine opioid abuse which is becoming endemic in the USA. Therefore, our results likely still underestimate the overall incidence of the high-risk behaviors.
Further studies will be required to define the rates of alcohol and substance abuse in pediatric patients with trauma. Studies using existing large databases (eg, National Trauma Data Bank) would be also limited by selection bias (as toxicology tests may not be uniformly ordered in pediatric patients) and screening with laboratory tests only. Therefore, a prospective multicenter cohort study will be ultimately required to answer this question. Ideally, such a study would include a broad range of social and geographical settings, universal screening using both laboratory tests and social history gathering as well as detailed analysis of patients’ demographics. It would also include opioid abuse.
The incidence of these behaviors, which was lowest at the age of 12, was associated with increasing age. As our study did not include patients younger than 12, it cannot ascertain whether there is any significant rate of alcohol and substance abuse in younger patients that would require screening. This study therefore supports the recommendation to screen all adolescent (starting at least at the age of 12) patients with trauma regardless of the severity injury as healthcare interactions for a minor injury may present an opportunity to prevent more severe injury in the future. Future studies should examine younger age groups as well as examine the cost/benefit ratio for specific test panels. As the rates of overall alcohol and drug use were higher than those computed from laboratory tests alone, we would recommend that screening should not only rely on laboratory testing but should also include specific history gathering by the providers.
Footnotes
Contributors: AAM contributed to the literature search, study design, data collection and data analysis. KAD was responsible for the study design. All authors contributed to the data interpretation, writing and critical revision of the manuscript.
Funding: The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests: None declared.
Patient consent: Not required.
Ethics approval: Institutional Review Board of the Yale School of Medicine.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1. Strong BL, Shipper AG, Downton KD, Lane WG. The effects of health care-based violence intervention programs on injury recidivism and costs: a systematic review. J Trauma Acute Care Surg 2016;81:961–70. doi:10.1097/TA.0000000000001222 [DOI] [PubMed] [Google Scholar]
- 2. Cordovilla-Guardia S, Vilar-López R, Lardelli-Claret P, Guerrero-López F, Fernández-Mondéjar E. Alcohol or drug use and trauma recidivism. Nurs Res 2017;66:399–404. doi:10.1097/NNR.0000000000000231 [DOI] [PubMed] [Google Scholar]
- 3. Nunn J, Erdogan M, Green RS. The prevalence of alcohol-related trauma recidivism: a systematic review. Injury 2016;47:551–8. doi:10.1016/j.injury.2016.01.008 [DOI] [PubMed] [Google Scholar]
- 4. Cordovilla-Guardia S, Fernández-Mondéjar E, Vilar-López R, Navas JF, Portillo-Santamaría M, Rico-Martín S, Lardelli-Claret P. Effect of a brief intervention for alcohol and illicit drug use on trauma recidivism in a cohort of trauma patients. PLoS One 2017;12:e0182441 doi:10.1371/journal.pone.0182441 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. COT ACS. Resources for optimal care of the injured patient. Chicago, Illinois: American College of Surgeons, Committee on Trauma, 2014. [Google Scholar]
- 6. Kelleher DC, Renaud EJ, Ehrlich PF, Burd RS. Pediatric Trauma Society Guidelines Committee. Guidelines for alcohol screening in adolescent trauma patients: a report from the Pediatric Trauma Society Guidelines Committee. J Trauma Acute Care Surg 2013;74:671–82. doi:10.1097/TA.0b013e31827d5f80 [DOI] [PubMed] [Google Scholar]
- 7. Nicolson NG, Lank PM, Crandall ML. Emergency department alcohol and drug screening for Illinois pediatric trauma patients, 1999 to 2009. Am J Surg 2014;208:531–5. doi:10.1016/j.amjsurg.2014.06.003 [DOI] [PubMed] [Google Scholar]
- 8. Martin KL, Vogt KN, Girotti MJ, Stewart TC, Parry NG. Drug use and screening in pediatric trauma. Ther Drug Monit 2011;33:439–42. doi:10.1097/FTD.0b013e318222d951 [DOI] [PubMed] [Google Scholar]
- 9. Gentilello LM, Rivara FP, Donovan DM, Jurkovich GJ, Daranciang E, Dunn CW, Villaveces A, Copass M, Ries RR. Alcohol interventions in a trauma center as a means of reducing the risk of injury recurrence. Ann Surg 1999;230:473 doi:10.1097/00000658-199910000-00003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Soderstrom CA, DiClemente CC, Dischinger PC, Hebel JR, McDuff DR, Auman KM, Kufera JA. A controlled trial of brief intervention versus brief advice for at-risk drinking trauma center patients. J Trauma 2007;62:1102–12. doi:10.1097/TA.0b013e31804bdb26 [DOI] [PubMed] [Google Scholar]
- 11. Underage drinking: why do adolescents drink, what are the risks, and how can underage drinking be prevented? Alcoholism NIoAAa A, ed Alcohol Alert, 2006. [Google Scholar]
- 12. Grant BF, Dawson DA. Age at onset of alcohol use and its association with DSM-IV alcohol abuse and dependence: results from the National Longitudinal Alcohol Epidemiologic Survey. J Subst Abuse 1997;9:103–10. doi:10.1016/S0899-3289(97)90009-2 [DOI] [PubMed] [Google Scholar]
- 13. Grant BF, Dawson DA. Age of onset of drug use and its association with DSM-IV drug abuse and dependence: results from the National Longitudinal Alcohol Epidemiologic Survey. J Subst Abuse 1998;10:163–73. doi:10.1016/S0899-3289(99)80131-X [DOI] [PubMed] [Google Scholar]
- 14. CDC) CfDCaP. Alcohol and Public Health: Alcohol-Related Disease Impact (ARDI). Average for United States 2006–2010 Alcohol-Attributable Deaths Due to Excessive Alcohol Use. 2017. https://nccd.cdc.gov/DPH_ARDI/Default/Report.aspx?T=AAM&P=f6d7eda7-036e-4553-9968-9b17ffad620e&R=d7a9b303-48e9-4440-bf47-070a4827e1fd&M=8E1C5233-5640-4EE8-9247-1ECA7DA325B9&F=&D= (accessed 12 Dec 2017).
- 15. Cunningham RM, Chermack ST, Ehrlich PF, Carter PM, Booth BM, Blow FC, Barry KL, Walton MA. Alcohol Interventions among underage drinkers in the ed: a randomized controlled trial. Pediatrics 2015;136:e783–93. doi:10.1542/peds.2015-1260 [DOI] [PMC free article] [PubMed] [Google Scholar]