

Abstract
The present study aims to investigate psychological stress and its determinants in Xinjiang field oil workers. Specifically, we aim to elucidate the mechanisms underlying psychological stress by comprehensively and quantitatively evaluating the processes involved in psychological stress, the factors which influence it, and their relationship.
The participants were 1200 field oil workers in Xinjiang who had been in service for at least 1 year. A structural equation model based on data from the symptom checklist, social support research scale, personality questionnaire, occupational burnout questionnaire, and occupational stress questionnaire was constructed to investigate the social (environmental) factors that influence physiological stress and the interplay among these factors.
The positive incidence of psychological stress in the field oil workers in Xinjiang was 12.54%. The structural equation model indicated that the main factors that influenced psychological stress in these workers included social support (0.077), occupational role (0.165), personal strain response (0.139), personality (0.189), and occupational burnout (0.380). Among these factors, occupational role, personality, and occupational burnout had a relatively strong predictive power for psychological stress reactions. The cortisol level in workers with positive psychological stress was significantly higher than that in workers with negative psychological stress.
Occupational stress, personality, and occupational burnout exert an impact on psychological stress in field oil workers. Therefore, interventions to address these factors should be taken to reduce the incidence of psychological stress.
Keywords: desert oil workers, occupational stress, psychological stress
1. Introduction
Psychological stress (PS) refers to a strained state in body and mind presenting as physiological and psychological reactions and resulting from inadequate personal ability or recognition during one's adaption to a lifestyle.[1,2] The emergence of PS can increase one's vigilance in coping with environmental changes. However, prolonged stress may cause serious damage to one's physical and mental health. In modern competitive society, people often encounter various stressful events, related to all kinds of daily events and to chronic and intensive occupational stress. These stressful events may cause psychological reactions including irritability, anxiety, depression, and insomnia, pervading a person's life. Dieserud et al[3] found that college suicide is mainly attributable to negative life events and loneliness in life. Het et al[4] reported that people under long-term stress are vulnerable to negative emotions such as compulsion, hostility, paranoia, anxiety, and depression, as well as interpersonal sensitivity and sleeping problems. Hence, it is important to recognize indications of stress in populations early on, and educate and counsel those who are afflicted, to prevent the development of a psychological disorder.
PS involves a dynamic process. Extensive research supports that stress and psychological reactions do not occur by way of a simple, “stimulus-response” causal relationship. The variables that influence PS are not only overlapping and repeating, but also interact with each other through mutual influence and restriction. Most past studies have focused on the relationship between a single factor and PS, such as the impact of social support or occupational stress on PS reactions. Such research lacks integrative and systematic study of the interplay between the many factors involved in PS.
The present investigation concerned the PS levels of field oil works in a special physical environment—the desert of Xinjiang. The factors that influence mild PS were evaluated based on the social support scale, personality questionnaire, occupational stress questionnaire, and symptom checklist. We used the structural equation model to construct a model of PS processes. Our study demonstrated the action mechanisms of PS-related personality, social support (an intermediate variable), and occupational stress (a direct variable). We comprehensively and quantitatively evaluated the process of PS, the influencing factors, and their interplay. Our work provides a basis for a comprehensive understanding of the mechanisms underlying PS.
2. Materials and methods
2.1. Study participants
According to the Occupation Catalogue of the People's Republic of China, cluster sampling was performed between June and October 2016. The subjects were from the Petroleum Administration Bureau in Xinjiang, China, which included 1326 field workers. The field workers were from 13 types of jobs including oil extraction, oil transportation, gas production, gas transportation, gathering pipelines, etc. Among these workers, 103 workers had <1 year of seniority and 23 were nonstaff for other reasons. Therefore, a total of 1200 oil workers were surveyed. In total, 1200 questionnaires were issued and 1150 questionnaires were returned, with a sample recovery rate of 95.83%. After excluding the incomplete questionnaires, 1100 effective questionnaires were obtained with an effective sample rate of 95.65%. The 1100 participants were between 22 and 59 years old (Mage 36.92 ± 7.41 years), including 637 males and 463 females, with service lengths of 2 to 36 (mean 16.73 ± 9.73) years. The education level of the majority of the workers (54.91%) was high school or junior college. The study protocol was approved by the Ethics Committee of Xinjiang Medical University (XJMU no. 20160214). Written informed consent was obtained from all participants.
2.2. Measurement of PS
The symptom checklist (SCL-90) was used here. This checklist contains 90 questions, and each question scores into 5 grades: 1 = absent, 2 = mild, 3 = moderate, 4 = relatively serious, and 5 = serious. A score of 1 is considered negative, and scores of 2 and above are considered to be positive symptoms. Higher scores indicate more severe symptoms. The 90 items in the checklist reflect the existence of 9 factors and 10 aspects related to mental symptoms or mental health, including somatization, compulsion, interpersonal sensitivity, depression, anxiety, hostility, phobia, paranoia, psychosis, and other problems. Based on our previous studies on the mental health status of oil workers, a unilateral 95% reference value was selected as the threshold:  .[5] A total score of 195.7 and above was considered to be positive, and the workers were assigned to the positive symptom group or the normal group accordingly.
.[5] A total score of 195.7 and above was considered to be positive, and the workers were assigned to the positive symptom group or the normal group accordingly.
2.3. Investigation of factors that influence PS
2.3.1. Evaluation of occupational stress
The occupational stress inventory (the revised edition, OSI-R) developed by Osipow and Spokane[6] in 1988 was used here. The OSI-R includes 3 questionnaires: the occupational role questionnaire (ORQ), the personal strain questionnaire (PSQ), and the personal resources questionnaire (PRQ). There is a total of 140 items in these 3 questionnaires, and each item scores into 5 grades. The final score reflects the intensity of occupational stress and stress response. There are 6 dimensions of the ORQ, 4 dimensions of the PSQ, and 4 dimensions of the PRQ, and each item weights 1 to 5 scores. A higher score in PRQ and PSQ indicates a higher level of occupational stress and a stronger stress response, whereas a higher score on the PRQ indicates a higher coping ability.
2.3.2. Evaluation of personality
We used the Chinese version of the Eysenck personality Questionnaire (EPQ) adapted by Yaoxian Gong (1983) to evaluate personality.[7] There are 85 items on this questionnaire, which are classified on 3 different dimensions and yield responses which together provide an inventory of one's personality. The EPQ includes the aspects of extraversion (E), neuroticism (N), and psychoticism (P). The tendencies toward these 3 dimensions constitute diverse personalities.
2.3.3. Evaluation of social support
The social support rating scale created by Shuiyuan[8] in 1986 was employed here. There are 10 questions pertaining to 3 dimensions in this scale: objective support (3 questions), subjective support (4 questions), and utilization of social support (3 questions). The internal consistency coefficient was between 0.89 and 0.94, and the reliability of repetitive tests was 0.92, indicating a good predictive validity. This scale well reflects the level of an individual's social support.
2.3.4. Evaluation of occupational burnout
The occupational burnout questionnaire, created by Li et al,[9] includes 3 aspects: emotional exhaustion, depersonalization, and reduced sense of accomplishment. There is a total of 15 items with 5 items for each dimension. This questionnaire scores in 7 grades: 1 for “strongly disagree” and 7 for “strongly agree.” Scores of 1 to 7 represent the agreement from a low to high level, with some of the items scoring the opposite way.
2.4. ELISA
Fasting peripheral blood (5 mL) was collected from 138 oil workers with positive PS and 138 age and gender matched oil workers with negative PS. Serum was isolated after centrifugation. Level of cortisol in the serum was measured with human cortisol ELISA kit (Cat. No. E-EL-H2464c; Elabscience Biotechnology Co, Ltd, Wuhan, China) according to the instructions.
2.5. Statistical analysis
The data were imported into the Epidata 3.1 database. The reliabilities of the questionnaires were assessed by calculating Cronbach α and intraclass correlation coefficient (ICC). The construct validity was analyzed by Root Mean Square Error of approximation (RMSEA), Non-normed fit index (NNFI/TLI), Comparative Fit Index (CFI), and goodness-of-fit index (GFI) through confirmatory factor analysis. The content validity was measured by item-total Pearson correlations coefficient. The categorical data were analyzed by chi-squared tests, and the quantitative data were analyzed by t tests. Multiple linear regressions of the general linear regression models were conducted using SPSS 13.0, and statistical model construction was performed in Lisrel 8.70 (Scientific Software International, Inc).
3. Results
3.1. Screening of positive symptoms of PS in field oil workers with different individual characteristics
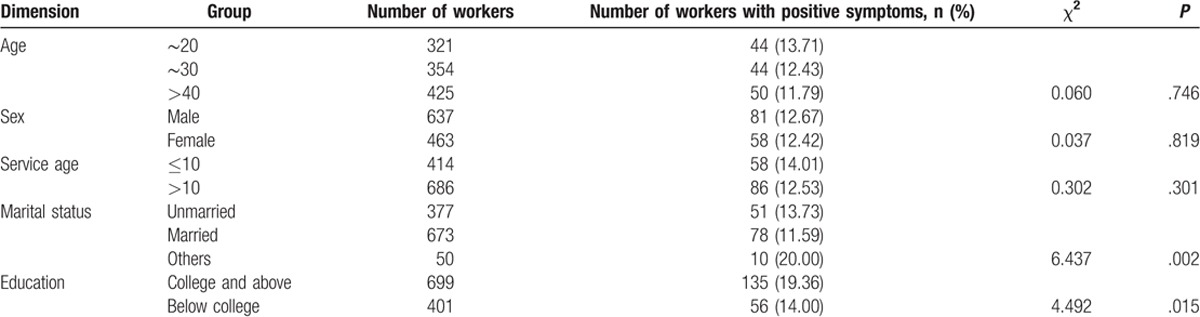
The validity and reliability of the questionnaires were satisfactory (Table 1). We used the SCL-90 to assess 1100 field oil workers. According to our previous study on the mental health status of oil workers, a unilateral 95% reference value of 195.7[5] was set as the threshold. A total score of 195.7 and above was considered positive, and the workers were assigned to the positive symptom group or the normal group accordingly. One hundred thirty-eight (approximately 12.54%) oil workers presented positive symptoms. The screening results of positive symptoms of PS in workers with different individual characteristics are shown in Table 2. The proportion of workers with positive symptoms did not significantly differ between the 3 age groups, between genders, or between service lengths (P > .05). The proportion of workers with positive symptoms in “other marital status” was significantly higher than that in the married and unmarried groups (P < .05), and the proportion in those with college and above education was significantly higher than that in those with below college education (P < .05). These results indicate that the proportion of workers with positive symptoms was distributed unevenly across marital status and educational level.
Table 1.
Reliability and validity of SCL-90, OSI-R, EPQ, SSRS, and occupational burnout.
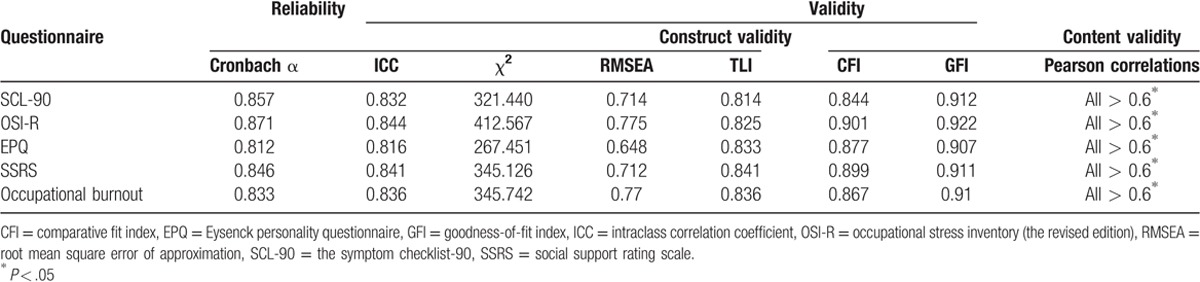
Table 2.
Screening of positive symptoms of psychological stress in workers with different individual characteristics.
3.2. Analysis of occupational stress in oil workers with different PS status
There was no significant difference in scores on the ORQ and PRQ between the normal group and the positive symptom group (both P > .05). The scores on the PSQ were significantly different between these 2 groups (P = .044), indicating the positive symptom group had greater personal strain.
As shown in Table 3, there was no significant difference in ORQ or PRQ scores between the 2 groups (P > .05). However, there was a significant difference between the 2 groups on PSQ scores (P = .044). This indicates that individuals in the positive symptom group had higher levels of personal strain.
Table 3.
Analysis of occupational stress in the positive symptom group and the normal group.

3.3. Personality traits in oil workers with different PS status
As shown in Table 4, the T scores for the E scale (extroversion–introversion), P scale (psychoticism), and L scales (lie) were not significantly different between the 2 groups (P > .05). The positive symptom group scored significantly higher on the N scale (neuroticism) compared with the normal group (P = .002). These results suggest that individuals prone to neuroticism are likely to develop unhealthy PS.
Table 4.
Personality traits in the positive symptom group and the normal group.

3.4. Analysis of social support in oil workers with different PS status
As shown in Table 5, the total social support score and objective support score were not significantly different between the positive symptom group and the normal group (P > .05). Subjective support and support utilization scores in the positive symptom group were significantly lower than those in the normal group. This indicates that social support was poor in the positive symptom group.
Table 5.
Analysis of social support in the positive symptom group and the normal group.

3.5. Analysis of occupational burnout in oil workers according to PS status
As shown in Table 6, the positive symptom group scored significantly higher in emotional exhaustion compared with the control group (P = .032). The scores in depersonalization and reduced sense of accomplishment were not significantly different between the 2 groups (P > .05). These results revealed that the positive symptom group was more likely to have unhealthy PS responses such as fatigue, irritability, and nervousness.
Table 6.
Analysis of occupational burnout in the positive symptom group and the normal group.

3.6. Multifactor logistic regression analysis of the influencing factors of PS
We conducted a stepwise logistic regression using presence of positive symptoms as a dependent variable. We used 25 factors related to various dimensions of work stress, personality, social support, and occupational burnout as predictor variables. There were 3 steps in the regression analysis, and in the last step, Nagelkerke R2 = 0.075, Hosmer–Lemeshow = 0.833. Both values were >0.05, suggesting that the model well fits the data. By taking the predictive probability of 0.5 as the cut-off point, the overall predictive accuracy was 62.70%. Finally, the regression equation included 7 independent variables (as listed in Table 7).
Table 7.
Multifactor logistic regression analysis of the influencing factors of psychological stress.

3.7. Construction of PS model in LISREL 8.70
To better visualize the interplay between the predisposing factors of PS, this study established a multivariate model of mild PS based on standard error of the mean. As shown in Table 8, the model fits well: the fitness indexes were RMSEA = 0.048, NFI = 0.949, and GFI = 0.906. Further analysis indicated that the coefficients between the influencing factors of PS were all statistically significant (T > 1.96), except for the influence of PRQ on SCL-90 scores and the influence of PSQ on occupational burnout. The main factors that influence PS included social support (0.077), occupational role (0.165), personal strain (0.139), personality (0.189), and occupational burnout (0.380). Of these variables, occupational role, personality, and occupational burnout were the factors with the most power for predicting PS reactions. In addition, work strain, social support, and personality impacts both SCL-90 scores and occupational burnout, while the path coefficient between occupational burnout and SCL-90 means was 0.38. This suggests that occupational burnout, as an intermediate variable, is correlated with PS responses and that it can regulate and control the development of unhealthy stress reactions.
Table 8.
Matrix of influence coefficients between the predisposing factors of psychological stress.

3.8. Comparison of cortisol level between workers with positive PS and those with negative PS
To further verify the results of subjective measurements obtained by questionnaires, we randomly selected 138 oil workers with positive PS and 138 age and gender matched oil workers with negative PS. The level of cortisol in the serum was detected by ELISA. The results showed that the cortisol level in workers with positive PS was 547.35 ± 94.96 mmol/L, significantly higher than that in workers with negative PS (517.91 ± 120.30 mmol/L; t = 2.633; P = .009). This result further confirmed the results of subjective measurements, suggesting that cortisol levels may be used as predictors of PS.
4. Discussion
In this study, 12.54% of the workers showed mental abnormality. In a study by Zhang et al[10] on 550 workers from 2 plants in Shanghai, 15.1% of the workers had a mental illness. Five studies on the depressive symptoms in professional populations using Zung's SDS scale showed that the detection rate of mental illness in the nursing staff was 37.1% to 47.4%[11]; the detection rate of mental illness in train attendants was 61.39%.[12] The rates of mental illness likely varied between these studies because they were performed in different decades with different testing tools and participants. In addition, the proportion of workers with positive symptoms of PS varied significantly in their marital status and level of education. This is probably because 90% of the field oil workers in this study are under cycles of field work (1–6 months) and the rest at home. They are in a monotonous working environment and exposed to the risk of occupational hazards such as concentrated hydrogen sulfide, fires, explosions, accidental mechanical injury, and oil spills. These risk factors and various burdens away from home lead to the emergence of PS reactions such as anxiety, depression, and problems with personal life (such as unhappy marriages), that can exacerbate the stress. Maslach et al[13–15] have reported that people with higher education have a higher level of work strain, self-imposed demand (self-expectation), and social expectations. When one's job does not meet one's expectations, one may experience stress reactions such as decreased job satisfaction and mental unhealthiness. These findings indicate that while PS exists universally, unique psychological characteristics form in different populations, work and life environments, and personalities. It is important to maintain mental health in the members of society and provide guidance to those with mental illness.
By comparing the occupational stress between the positive symptom group and the control group, our study found that the positive symptom group scored higher on personal strain than did the control group. In the logistic regression analysis, personal strain and self-care entered into the equation, suggesting that these 2 factors can predict the occurrence of PS. Specifically, individuals who had less self-care and greater reactions to occupational stress were susceptible to psychological problems such as depression and anxiety. The results of the present study are similar to the theories of Selye,[16] which indicated that more than half of human illnesses related to strain and overstrain can lead to psychogenic mental disorders. Occupational stress is a special type of stress. Unlike biological, physical, or chemical factors that can cause specific occupational diseases, occupational stress damages physical and mental health in a nonspecific way, and can lead to or induce the pathogenesis of coronary disease, hypertension, peptic ulcers, and neurasthenic syndrome, therefore increasing absenteeism, reducing work efficiency, and even causing accidents.[17–20] In Japan, 60% of absenteeism is due to “overwork” that is caused by long-term physical and mental stress. The relationship between occupational stress and mental illness has been demonstrated in the association of stress factors such as high work pressure, strict supervisory control, lack of autonomy, and lack of transparency with psychological problems like anxiety and depression.[21] In addition, occupational stress can also cause behavioral changes such as excessive smoking, alcoholism, negative emotion, lack of confidence, decreased energy, frequent medical visits, drug dependence, and unwillingness to participate in social activities.[22–24] Thus, reducing occupational stress and improving self-care and psychological adjustment are a key way to prevent PS.
Social support has been found to strongly predict mental health status and has an enduring effect on it.[25] The findings in this study show that subjective support and support utilization has a buffering effect on PS reactions. The positive symptom group had significantly less subjective support and support utilization than the control group. Multifactor logistic regression analysis of the factors that influenced PS indicated that support utilization makes a remarkable contribution to the buffering of PS reactions. Social support can be classified into 2 categories. One category is objective, visible, or practical support, that is, available material support and contacts with others, and the extent to which it can be utilized. The other is subjective or perceived emotional support, like the emotional satisfaction that accompanies social respect, and being supported and understood. This category is largely based on subjective feelings. Researchers have different opinions on the importance of these 2 types of support, but most researchers believe that perceived support is more meaningful than objective support. Although perceived support may not be objective reality, because “perceived reality is indeed the psychological reality,” the psychological reality acts as the realistic (intermediate) variable that impacts personal behavior and development. Hence, support is very important for mental health no matter if it is from an organization, society, or family. Perceived support is more effective than material support. Moreover, encouraging support utilization can help prevent the occurrence of PS reactions.
Personality refers to the stable psychological and behavioral characteristics of a person. Personality is a determining factor that leads to different reactions in different people, to the same stress situation.[26–28] Holeva and Tarrier[29] surveyed 256 victims of traffic accidents using EPQ, and the results showed that the individuals prone to neuroticism and psychoticism had higher levels of tension and anxiety, which are often symptoms of mental illness. Aidman and Kollaras-Mitsinikos’ study indicated that extroverted individuals had a higher likelihood of suffering from post-traumatic stress disorder.[30] In this study, a comparison of the EPQ scores of the positive symptom group versus the control group showed that the dimension of neuroticism varied between the groups, such that highly neurotic individuals had higher degrees of PS. In the present study, a comparison of the EPQ scores of the positive symptom group versus the control group showed that the dimension of neuroticism varied between the groups, such that the highly neurotic individuals had significantly higher degrees of PS. This is consistent with the findings of Ogle et al,[31] which suggested that high neuroticism is a critical factor for the development of stress disorders. In other words, people who are prone to anxiety, easily excited or depressed, show strong emotional reactions (and in some cases, even irrational behavior) have higher degrees of PS. Our analysis to predict PS reactions revealed that the risk of mental illness in individuals with high levels of neuroticism (N) and psychoticism (P) was 1.512-fold and 1.055-fold, respectively, compared with those without high scores on these 2 dimensions.
According to the definition by Freudenberger, a clinical psychologist in the United States, job burnout is a state of physical and mental exhaustion when a person cannot effectively relieve work pressure or properly cope with the setbacks of work.[32] The core components include 3 dimensions: emotional exhaustion, depersonalization, and low sense of accomplishment. A study by Luo and Khamisa, N showed that job burnout has a linear relationship with mental health.[33,34] In this study, the positive symptom group scored higher in emotional exhaustion than the control group, and the multifactor logistic regression analysis of the influencing factors on PS also showed that emotional exhaustion was a predictive factor for mental illness.
In recent years, Qianjin[35] has carried out multifactor analysis of the influencing factors of stress reactions. Their study demonstrates that the stress process, which involves diverse factors, is indeed an interaction system of multiple factors that are overlapping and redundant in nature. It employed a structural equation model to mimic the relationship between PS and its influencing factors in field oil workers in Xinjiang. This model verified the previous findings and quantified the relation between the influencing factors. The results indicated that occupational role, social support, and personality were the major factors that influenced PS. In addition, occupational stress was an important factor that led to occupational burnout, the outcome of which was the occurrence of PS reactions (such as depression). During this process, personality and social support can mitigate or aggravate the severity of mental illness.
The hypothalamic–pituitary–adrenal axis is a neuroendocrine system involved in the regulation of stress response.[36] Stress response is triggered by the activation of the hypothalamic–pituitary–adrenal axis, causing release of corticotrophin releasing hormone, adrenocorticotrophic hormone, and cortisol release.[37] Therefore, the level of cortisol to some extent reflects the level of PS.[38] In this study, we found that the cortisol level in workers with positive PS was significantly higher than that in workers with negative PS. These data further confirmed that the results of subjective measurements obtained by questionnaires and indicate that cortisol levels may be used as predictors of PS.
This study has several limitations. First, we collected the information by on-site questionnaire surveys and self-reported PS, and the mental reactions were influenced by individual subjective factors, which may have yielded report bias. Second, some potential confounding factors such as income, policies, organization, and working atmosphere were not taken into account in this survey. Third, this report was a cross-sectional study and only investigated the effect of social environmental factors on PS. The influence of invariant factors (such as gene polymorphisms) on the risk of PS was not investigated in this study. Further studies are warranted.
5. Conclusion
Occupational stress, personality, and occupational burnout exert an impact on PS in field oil workers. Therefore, interventions to address these factors should be taken to reduce the incidence of PS.
Author contributions
Li Ning: Wrote the manuscript and Analyzed the data.
Suzhen Guan: Epidemiological Investigation.
Jiwen Liu: Conceived and designed the experiments and Technical Support.
Conceptualization: Jiwen Liu.
Data curation: Suzhen Guan.
Funding acquisition: Jiwen Liu.
Supervision: Suzhen Guan, Jiwen Liu.
Writing – review & editing: Li Ning.
Footnotes
Abbreviations: E = extraversion, EPQ = Eysenck personality questionnaire, N = neuroticism, ORQ = occupational role questionnaire, OSI-R = occupational stress inventory (the revised edition), P = psychoticism, PRQ = personal resources questionnaire, PS = psychological stress, PSQ = personal strain questionnaire, SCL-90 = the symptom checklist-90.
This study was supported by the Xinjiang Uygur Autonomous Region Natural Science Foundation (2015211C013).
The authors have no conflicts of interest to disclose.
References
- [1].Cohen S, Janicki-Deverts D, Miller GE. Psychological stress and disease. JAMA 2007;298:1685–7. [DOI] [PubMed] [Google Scholar]
- [2].Appley MH, Trumbull R. Psychological Stress. New York, NY: Appleton-Century-Crofts; 1967. [Google Scholar]
- [3].Dieserud G, Forsén L, Braverman MT, et al. Negative life events in childhood, psychological problems and suicide attempts in adulthood: a matched case-control study. Arch Suicide Res 2002;6:291–308. [Google Scholar]
- [4].Het S, Schoofs D, Rohleder N, et al. Stress-induced cortisol level elevations are associated with reduced negative affect after stress: indications for a mood-buffering cortisol effect. Psychosom Med 2012;74:23–32. [DOI] [PubMed] [Google Scholar]
- [5].Li N. The norm establishment of symptom checklist 90 in Chinese Han population in Xinjiang area. Chinese J Occup Med 2012;39:8–12. [Google Scholar]
- [6].Osipow SH, Spokane AR. Occupational Stress Inventory—Revised. 1998;Odessa, FL: Psychological Assessment Resources, 1–15. [Google Scholar]
- [7].Yaoxian G. Hunan Medical College, Eysenck Personality Questionnaire (Revised). Changsha:1986. [Google Scholar]
- [8].Shuiyuan X. Theoretical basis and application of social support rating scale. J Clin Psychiatry 1994;4:98–100. [Google Scholar]
- [9].Fuye L, Jiwen L. The reliability and validity of the measurement tool for the mental fatigue of ET. Chinese J Occup Health Occup Dis 2009. 156–9. [Google Scholar]
- [10].Hunan Science and Technology Press; 1998;Mingyuan Z. Handbook of Psychiatric Rating Scale. [Google Scholar]
- [11].Jing C, Bing B. Mental health status and research progress of nurses in China. Nurs Res 2003;17:563–4. [Google Scholar]
- [12].Wang YB, Cui JL, Qin L, et al. Correlation analysis between self-rated health and depression and anxiety of railway workers in key sectors. Occup Health 2010;18:1. [Google Scholar]
- [13].Maslach C, Schaufeli WB, Leiter MP. Job burnout. Annu Rev Psychol 2001;52:397–422. [DOI] [PubMed] [Google Scholar]
- [14].Chickering AW, Dalton JC, Stamm L. Encouraging Authenticity and Spirituality in Higher Education. New York, NY: John Wiley & Sons; 2015. [Google Scholar]
- [15].Nabirye RC, Brown KC, Pryor ER, et al. Occupational stress, job satisfaction and job performance among hospital nurses in Kampala, Uganda. J Nurs Manag 2011;19:760–8. [DOI] [PubMed] [Google Scholar]
- [16].Butterworth-Heinemann, Selye H. Stress in Health and Disease. 2013. [Google Scholar]
- [17].Kivimäki M, Kawachi I. Work stress as a risk factor for cardiovascular disease. Curr Cardiol Rep 2015;17:74. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [18].BMJ Publishing Group Ltd, Netterstrøm B. Job Strain and Hypertension. 2014. [Google Scholar]
- [19].Melinder C, Udumyan R, Hiyoshi A, et al. Decreased stress resilience in young men significantly increases the risk of subsequent peptic ulcer disease—a prospective study of 233 093 men in Sweden. Aliment Pharmacol Ther 2015;41:1005–15. [DOI] [PubMed] [Google Scholar]
- [20].Loriol M. A sociological stance on fatigue and tiredness: social inequalities, norms and representations. Neurophysiol Clin 2017;47:87–94. [DOI] [PubMed] [Google Scholar]
- [21].Huang GD, Feuerstein M, Sauter SL. Occupational stress and work-related upper extremity disorders: concepts and models. Am J Ind Med 2002;41:298–314. [DOI] [PubMed] [Google Scholar]
- [22].Dalgaard L, Eskildsen A, Carstensen O, et al. Changes in self-reported sleep and cognitive failures: a randomized controlled trial of a stress management intervention. Scand J Work Environ Health 2014;40:569–81. [DOI] [PubMed] [Google Scholar]
- [23].Velez MJ, Neves P. Abusive supervision, psychosomatic symptoms, and deviance: can job autonomy make a difference? J Occup Health Psychol 2016;21:322–33. [DOI] [PubMed] [Google Scholar]
- [24].Bakker AB, Costa PL. Chronic job burnout and daily functioning: a theoretical analysis. Burnout Res 2014;1:112–9. [Google Scholar]
- [25].Lee Y. The predictive value of self assessed general, physical, and mental health on functional decline and mortality in older adults. J Epidemiol Community Health 2000;54:123–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [26].Kardum I, Krapić N. Personality traits, stressful life events, and coping styles in early adolescence. Pers Individ Dif 2001;30:503–15. [Google Scholar]
- [27].Harvey CJ, Gehrman P, Espie CA. Who is predisposed to insomnia: a review of familial aggregation, stress-reactivity, personality and coping style. Sleep Med Rev 2014;18:237–47. [DOI] [PubMed] [Google Scholar]
- [28].Zhou YY, Li DP, Li X, et al. Big five personality and adolescent internet addiction: the mediating role of coping style. Addict Behav 2017;64:42–8. [DOI] [PubMed] [Google Scholar]
- [29].Holeva V, Tarrier N. Personality and peritraumatic dissociation in the prediction of PTSD in victims of road traffic accidents. J Psychosom Res 2001;51:687–92. [DOI] [PubMed] [Google Scholar]
- [30].Aidman EV, Kollaras-Mitsinikos L. Personality dispositions in the prediction of posttraumatic stress reactions. Psychol Rep 2006;99:569–80. [DOI] [PubMed] [Google Scholar]
- [31].Ogle CM, Siegler IC, Beckham JC, et al. Neuroticism increases PTSD symptom severity by amplifying the emotionality, rehearsal, and centrality of trauma memories. J Pers 2017;85:702–15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [32].Freudenberger HJ. Staff burn-out. J Soc Issues 1974;30:159–65. [Google Scholar]
- [33].Luo H, Yang H, Xu XJ, et al. Relationship between occupational stress and job burnout among rural-to-urban migrant workers in Dongguan, China: a cross-sectional study. BMJ Open 2016;6:e012597. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [34].Khamisa N, Oldenburg B, Peltzer K, et al. Work related stress, burnout, job satisfaction and general health of nurses. Int J Environ Res Public Health 2015;12:652–66. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [35].Qianjin J. A comprehensive evaluation of psychosocial stress factors. Chinese Behav Med Sci 1998;7:182–4. [Google Scholar]
- [36].Crowley SK, O’Buckley TK, Schiller CE, et al. Blunted neuroactive steroid and HPA axis responses to stress are associated with reduced sleep quality and negative affect in pregnancy: a pilot study. Psychopharmacology (Berl) 2016;233:1299–310. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [37].Janssens H, Clays E, Fiers T, et al. Hair cortisol in relation to job stress and depressive symptoms. Occup Med (Lond) 2017;67:114–20. [DOI] [PubMed] [Google Scholar]
- [38].Caparros-Gonzalez RA, Romero-Gonzalez B, Strivens-Vilchez H, et al. Hair cortisol levels, psychological stress and psychopathological symptoms as predictors of postpartum depression. PLoS ONE 2017;12:e0182817. [DOI] [PMC free article] [PubMed] [Google Scholar]