

Abstract
Aim
The aim of the study was the subjective assessment of the quality of life (QoL) of 140 patients treated with dialysis (peritoneal dialysis and hemodialysis).
Background
Chronic kidney disease and the methods of its treatment play an important part in shaping the QoL of patients receiving dialysis. As a result, kidney failure causes many limitations in patients’ physical, mental, and social activities.
Methods
The instrument to measure the QoL was the authors’ own questionnaire made on the basis of Kidney Disease and Quality of Life Short Form version 1.2 (KDQOL – SF 1.2) and their selection of areas influencing the perceived QoL of chronically ill patients.
Results
The research showed that patients receiving peritoneal dialysis assessed their QoL in its different dimensions as much higher than patients receiving hemodialysis. The parameter having the biggest negative impact on the QoL of patients receiving hemodialysis was an impeded possibility to continue work or studies and a change of life plans. The will to live was more highly assessed by patients receiving peritoneal dialysis as compared to patients receiving hemodialysis.
Conclusion
In order to improve the functioning of hemodialysis patients in a manner most similar to healthy persons, the renal replacement therapy should consider patients’ individual needs and expectations, ie, guarantee flexible hours of work or study and of receiving dialysis. In addition, patients treated with hemodialysis should receive psychological care, in particular those demonstrating emotional problems, in order to achieve better results in therapy and improve their QoL.
Keywords: hemodialysis, negative symptoms, peritoneal dialysis, renal failure, renal replacement therapy, quality of life
Introduction
Based on different epidemiological data, chronic kidney disease affects on average 10% of the population around the world. This is the result of the aging of the population and the increase of civilization diseases such as diabetes, hypertension or obesity.1–3 However, the availability of renal replacement therapy around the world is very diverse and depends first of all on a country’s financial resources. In Poland, over 25,000 patients receive renal replacement treatment, of which about 33% are patients with active transplanted kidneys, about 58% are patients receiving hemodialysis, and 5% are those receiving peritoneal dialysis. Taking into account only the dialysis therapy, in Poland about 92% of patients receive hemodialysis while about 8% of patients receive peritoneal dialysis.4–7 Life of patients with chronic kidney disease becomes reorganized and adapted to changes resulting from the nature of the disease and the methods of its treatment. What is more, patients are dependent on the dialysis apparatus and the medical personnel.5,8 The treatment also involves limitations in the manner of eating and drinking as well as in physical activities.5,9,10 In turn, the intensity of mental and somatic symptoms largely affects the level of the quality of life (QoL) as perceived by patients. At the same time, the occurrence of the negative symptoms of dialysis therapy (such as pain, sleep disorder, depression, the weakening of fluctuations in blood pressure, and stomach ache) or limitations resulting from the illness, reduce the QoL and cause the illness to be perceived as burdensome. Also, the professional activity of patients changes, which consequently worsens their material situation. Patients suffering from chronic kidney disease also give up other activities, such as sport, hobbies, social activities, and personal development.11–13 The QoL of patients suffering from chronic kidney disease is shaped through social and family relationships. Not only family but also good social relationships are of great importance and are the source of positive feelings and self-esteem and improve the QoL. On the other hand, a lack of support and acceptance from family and friends has a negative influence on patients’ health through lower self-esteem, and feelings of hopelessness and helplessness, all of which causes lower mood, depression, feelings of resignation, and a sense of life meaning less.12,14 What is more, before the selection of the method of renal replacement therapy, patients should be thoroughly informed of any possible methods of treatment, without pressurizing them to select or reject a particular method. The selection of a method should be an independent, conscious and optimal decision for patients.5,15 Patients’ QoL is also influenced by the quality of medical care and that of the closest environment, including the level of professional qualifications and experience of the medical personnel. Patients require directed medical rehabilitation and education to cope with the disease and the manner of treatment and to prevent complications. Patients receiving chronic dialysis should receive holistic care, taking into account somatic, mental, and social aspects, which can consequently prolong life and decrease their mortality.9,15
Patients and methods
The study was conducted between 2013 and 2014. The research group were 140 patients receiving dialysis therapy due to chronic kidney failure. Only the Polish population was included in the study. From the Clinic of Nephrology and Dialysis in Warsaw, 100 patients receiving renal replacement therapy were selected, of whom 60 received hemodialysis (hemodialysis was carried out in a dialysis station – 3 times a week for 4–5 hours) and the rest received peritoneal dialysis (peritoneal dialysis was conducted at home and changes were done manually). In contrast, the remaining 40 patients received hemodialysis (3 times a week for 4–5 hours) in the State Clinical Hospital of the Infant Jesus in Warsaw. Patients consciously and voluntarily agreed to participate in the research. The study included patients who gave informed, non-written consent to participate (oral consent). The author’s questionnaire was made for the purpose of the research and estimated the subjective QoL of patients receiving renal replacement therapy. The questionnaire was made based on a standardized instrument of Kidney Disease and Quality of Life Short Form version 1.2 (KDQOL – SF 1.2) (used as a basis to create a modified questionnaire) and consisted of two parts. The KDQOL – SF 1.2 questionnaire, was translated and validated for the Polish language.
The first part included basic information on patients, such as sex, age, type and time of dialysis, the influence of the treatment on any changes of life and somatic symptoms caused by renal replacement therapy. The second part of the questionnaire was the analysis of well-being of patients receiving dialysis, in which a scale of points from 1 to 10 was used, where number 1 indicated the lowest level of emotions, while number 10 indicated the highest. In order to determine the strength of relationships and correlations between the researched variables, the chi-square test was used, and the level of statistical significance was set at p<0.05.
In accordance with the statement of the Ethical Committee of the Medical University of Warsaw: “The Committee does not provide opinions on surveys, retrospective studies, or other non-invasive research”, the ethical committee’s consent for the presented research was not required.16
Results
The respondents (N=140) were divided into four age groups. Patients aged over 64 years (40% of those who received hemodialysis and 45% of those who received peritoneal dialysis) were the biggest group of respondents, while the smallest group were patients between 18 and 33 years of age (of whom 6% received hemodialysis and 10% received peritoneal dialysis). The results showed that age difference between the analyzed groups was not statistically significant. They also showed that the most often used method of treatment for chronic kidney failure in the male group of respondents, was hemodialysis (61%), while in the female group of respondents, it was peritoneal dialysis (52.5%). In contrast, the smallest group of patients were women receiving hemodialysis (39%) and men receiving peritoneal dialysis (47.5%), see Table 1 and Figure 1. Also in this case, there were no statistically significant differences found between the groups of respondents.
Table 1.
Patient characteristics by age groups (N=140)
| Group | Age group (years)
|
Totals | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 18–33
|
34–48
|
49–63
|
≥64
|
|
||||||
| n=10 | % | n=28 | % | n=44 | % | n=58 | % | n=140 | % | |
| Hemodialysis | 6 | 6 | 23 | 23 | 31 | 31 | 40 | 40 | 100 | 71.5 |
| Peritoneal dialysis | 4 | 10 | 5 | 12.5 | 13 | 32.5 | 18 | 45 | 40 | 28.5 |
Notes: χ2=2, 4; df=3; p=0.49.
Figure 1.
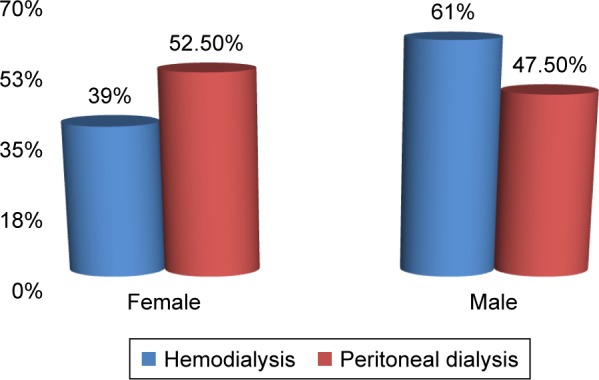
Characteristics of the studied group by sex.
The dominant causes of chronic renal failure are glomerulonephritis, hypertensive nephropathy, and diabetic nephropathy. Accompanying diseases include cardiovascular diseases, obesity, diabetic retinopathy, neuropathy, inflammation, and systemic diseases.
The influence of dialysis on change of lifestyle
The presented data show that patients receiving hemodialysis experienced most changes in their everyday lives. The changes were related to the influence of dialysis on the continuation of work or studies (41%) and life plans (72%), and the percentage was higher than in the case of patients receiving peritoneal dialysis. This relationship between the two groups of patients and the influence on the continuation of work and the change of life plans was statistically significant.
Complications occurring as a result of chronic renal replacement therapy
The research assessed the frequency of complications occurring during dialysis. Patients receiving hemodialysis usually pointed to muscle spasms (very often: 18%, often: 21%), skin dryness and itching (very often: 21%, often: 22%) and an increase or decrease in blood pressure (very often: 29%, often: 27%). Patients receiving peritoneal dialysis demonstrated identical symptoms but they experienced them to a lesser degree, ie, muscle spasms (very often: 18%, often: 21%), skin dryness and itching (very often: 22.5%, often: 12. 5%) and an increase or decrease in blood pressure (very often: 10%, often: 10%). At the same time, among the analyzed variables, statistically significant relationships were shown between the increase and the decrease in blood pressure and the groups of respondents. However, no significant correlations were found in the analysis of the remaining symptoms being the result of the dialysis therapy (Table 2). It was also shown that patients receiving hemodialysis noted the following symptoms more frequently than patients receiving peritoneal dialysis: sleep disorder (very often: 30%, often: 19%), feeling pain (very often: 15%, often: 17%) and difficulties in sexual life (very often: 4%, often: 6%). At the same time, significant differences were observed between patients receiving hemodialysis and patients receiving peritoneal dialysis in terms of sleep disorder and feeling pain (Table 3).
Table 2.
The incidence of complications during dialysis (N=140)
| Complications (variables) | The incidence of complications (%)
|
p-value | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Very often
|
Often
|
Sometimes
|
Rarely
|
Very rarely
|
Never
|
||||||||
| HD | PD | HD | PD | HD | PD | HD | PD | HD | PD | HD | PD | ||
| Dizziness | 5 | 2.5 | 6 | 7.5 | 19 | 12.5 | 24 | 20 | 14 | 25 | 32 | 32.5 | 0.541 |
| Impaired vision | 6 | 2.5 | 14 | 7.5 | 17 | 10 | 17 | 25 | 19 | 10 | 27 | 45 | 0.13 |
| Fainting | 3 | 0 | 4 | 5 | 20 | 12.5 | 19 | 15 | 18 | 12.5 | 36 | 55 | 0.365 |
| Muscle cramps | 18 | 15 | 21 | 17.5 | 33 | 20 | 13 | 12.5 | 8 | 15 | 7 | 20 | 0.163 |
| Chest pain | 4 | 0 | 5 | 7.5 | 13 | 5 | 14 | 15 | 18 | 17.5 | 46 | 55 | 0.532 |
| Dryness and itching | 21 | 22.5 | 22 | 12.5 | 24 | 15 | 9 | 15 | 5 | 10 | 19 | 25 | 0.418 |
| Dyspnoea | 4 | 5 | 11 | 5 | 17 | 12.5 | 19 | 10 | 16 | 10 | 33 | 57.5 | 0.266 |
| Nausea | 5 | 2.5 | 12 | 2.5 | 16 | 17.5 | 10 | 15 | 17 | 10 | 40 | 52.5 | 0.37 |
| Edema | 3 | 5 | 15 | 7.5 | 29 | 27.5 | 21 | 12.5 | 7 | 22.5 | 25 | 25 | 0.121 |
| An increase or decrease in blood pressure | 29 | 10 | 27 | 10 | 25 | 37.5 | 11 | 22.5 | 7 | 10 | 1 | 10 | 0.002 |
Abbreviations: HD, hemodialysis; PD, peritoneal dialysis.
Table 3.
Incidence of symptoms after dialysis (N=140)
| Ailments (variables) | The incidence of ailments (%)
|
p-value | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Very often
|
Often
|
Sometimes
|
Rarely
|
Very rarely
|
Never
|
||||||||
| HD | PD | HD | PD | HD | PD | HD | PD | HD | PD | HD | PD | ||
| Increased fatigue | 13 | 5 | 31 | 32.5 | 34 | 30 | 16 | 25 | 2 | 7.5 | 4 | 0 | 0.268 |
| Sleep disorders | 30 | 5 | 19 | 12.5 | 17 | 25 | 8 | 15 | 8 | 17.5 | 18 | 25 | 0.019 |
| Pain | 15 | 0 | 17 | 5 | 27 | 25 | 22 | 27.5 | 10 | 30 | 9 | 12.5 | 0.007 |
| Decreased appetite | 5 | 2.5 | 11 | 10 | 17 | 25 | 11 | 2.5 | 9 | 12.5 | 47 | 47.5 | 0.528 |
| Problems in sexual life | 4 | 0 | 6 | 0 | 8 | 25 | 8 | 7.5 | 6 | 10 | 68 | 57.5 | 0.144 |
Abbreviations: HD, hemodialysis; PD, peritoneal dialysis.
Perceiving limitations by patients receiving chronic dialysis therapy
Our research concluded that peritoneal dialysis caused the least number of limitations in drinking and eating, which referred to 50% and 30% of respondents, respectively. It also did not limit the possibility for travel for 27.5% respondents. In contrast, 37.5% of patients receiving hemodialysis felt significant dependence on the medical personnel. In turn, statistically significant differences were observed between the respondents and their limitations in drinking and eating and dependence on the medical personnel. In contrast, significant limitations in drinking were suffered by patients receiving hemodialysis (20%). This group of patients showed significant dependence on the medical personnel (28%). The type of received dialysis and limitations in drinking as well as the dependence on the medical personnel were statistically significant (Table 4).
Table 4.
Factors significantly affecting the perception of restrictions by patients undergoing dialysis (N=140)
| Patients | Fluid intake (%) | Eating foods (%) | Traveling (%) | Medical staff (%) |
|---|---|---|---|---|
| Hemodialysis (n=100) | 20 | 5 | 26 | 28 |
| Peritoneal dialysis (n=40) | 0 | 5 | 20 | 2.5 |
| p-value | 0.000 | 1 | 0.3 | 0.000 |
Mental health and the emotional state of patients receiving dialysis therapy
The sense of life meaning (37.5%) and the patients’ will to live (47.5%) were more often selected by patients receiving peritoneal dialysis than by patients receiving hemodialysis. However, variables related to joy and the sense of life meaning as combined with the type of received dialysis were not statistically significant. One variable that was assessed more highly by patients receiving peritoneal dialysis was the will to live. The biggest percentage of patients fearing for their future referred to patients receiving peritoneal dialysis: 22.5%, while patients receiving hemodialysis more often indicated aggression: 8% and anxiety: 4%. Variables such as the level of anxiety, aggression, and fear for the future did not show significant correlations, both in patients receiving hemodialysis and in those receiving peritoneal dialysis.
Discussion
Treating chronic kidney failure is related to receiving long-term dialysis therapy by patients. Both hemodialysis and peritoneal dialysis significantly change patients’ lives. The objective of measurement of the QoL of patients receiving dialysis was to compare and show the overall picture of treatment. The research by Dutkowska et al8 showed that both in the first and in the second group of respondents, the most common complications were muscle spasms and skin itching. In turn, patients receiving hemodialysis more often experienced back pain, headache, and increased blood pressure. They also indicated a higher onerousness factor related to receiving dialysis. In contrast, patients receiving peritoneal dialysis more often experienced nausea, vomiting, chills, and increased temperature. Metanalyses and work conducted in other countries have shown that QoL does not differ substantially between the two groups.17 In another study that has been published, authors have noticed differences in particular domains of QoL, such as pain and social interaction.18 Another study proved that daily nocturnal hemodialysis allows for greater flexibility to work and to take part in leisure and daily activities, as well as maintaining better blood pressure and weight control, with less water intake limitation.19 In turn, Kapka-Skrzypczak et al9 confirmed that in the minimalization of limitations related to received dialysis and in creating better QoL, patients receiving peritoneal dialysis gained a significant advantage. In contrast, patients receiving hemodialysis more often experienced worse quality of sleep, chronic fatigue, pain, and vomiting. Similar results were obtained by Turkmen et al20 and Theofilou21 who showed that in a group of patients receiving hemodialysis 41%–83% experienced sleep disorder and chronic weakness. In contrast, two other studies22,23 proved that patients receiving hemodialysis had fewer sleep problems than patients receiving peritoneal dialysis. Sapilak et al24 based on a 3-year observation of 418 patients pointed out a significant reduction in QoL, in particular in physical activity and in everyday activities. Also, García-Llana et al25 and Arenas et al26 showed worse physical activity in a group of patients receiving hemodialysis. What is more, Gonçalves et al23 pointed to the increase of discomfort in the sexual area of patients receiving peritoneal dialysis and their partners, which was most likely the result of implantation of the catheter into their abdomen. However, another research study did not show any significant differences in sexual activity between patients receiving peritoneal dialysis and those receiving hemodialysis.27 In contrast, our own research showed that patients receiving hemodialysis more often complained about muscle spasms of legs, skin dryness and itching, and fluctuations in blood pressure than patients receiving peritoneal dialysis. What is more, the quality of sleep, experiencing pain, and problems in sexual activity were also worse in patients receiving hemodialysis.
The subject of many studies on the QoL of patients receiving chronic dialysis is also the influence of well-being, the level of positive and negative emotions, and mood disorders. The majority of published data shows strong weakening of the QoL of patients receiving hemodialysis. Patients receiving peritoneal dialysis and healthy persons presented the lowest levels of the analyzed features. Similar results were obtained in other studies.23,26 However, the literature differs as to the physical activities of patients receiving peritoneal dialysis and hemodialysis. Misiewicz et al28 reported psychosocial problems in patients receiving chronic hemodialysis and they found that the most frequent emotions experienced by this group of patients were despondency, resignation, and helplessness – all factors characteristic for depression.
A disturbing fact was that a given type of treatment caused anxiety in patients in connection with too many duties and a lack of control over their lives. In turn, Sapilak et al24 in their studies on personality profile and mood disorder of patients receiving hemodialysis showed the existence of depression and anxiety of mild, moderate and severe nature in the analyzed group of patients. In addition, a strong correlation was observed between a given type of personality and the severity of symptoms of anxiety and depression. The disorders developed more frequently in patients with a negative attitude toward their situation, who did not try to cope with their new problems. Other studies29,30 have shown that patients receiving hemodialysis and at the same time being treated by a clinical psychologist perceived their QoL higher and showed higher parameters in mental health.
In contrast, Makara-Studzińska et al31 in their studies on depressive disorders in patients suffering from end stage renal disease showed that patients receiving peritoneal dialysis most frequently suffered from depression. In contrast, the analysis of our own research showed that despite a lack of correlations, patients receiving hemodialysis more frequently experienced negative emotions, such as anxiety and aggression than patients receiving peritoneal dialysis. However, patients receiving hemodialysis to a lesser degree experienced fear for their future as compared to the other group of patients. This is most likely related to resignation and a lack of strong will to take up new, although hard challenges related to chronic dialysis therapy were predominant in these patients. What is more, the research showed that patients receiving peritoneal dialysis more often indicated a greater will to live than patients receiving hemodialysis. In turn, the sense of life meaning and joy were higher in patients receiving peritoneal dialysis. Similar results were obtained by Zhang et al32 who proved that patients receiving peritoneal dialysis have a better social life. Another important factor to influence the QoL of patients receiving dialysis was the possibility to travel. Misiewicz et al28 showed that over 80% of patients receiving hemodialysis gave up travelling during the course of the disease and that patients’ attachment to a given dialysis unit limited travelling, mainly due to the necessity to receive dialysis in another unit. Own research showed similar results confirming that patients receiving hemodialysis felt limitations related to longer travelling outside the dialysis unit more frequently than patients receiving peritoneal dialysis. The research studied the differences between the type of dialysis and patients’ limitations in eating and drinking and the degree of patients’ dependence from the medical personnel. It was proved based on the research that patients receiving peritoneal dialysis experienced eating limitations and dependence from the medical personnel to a lesser degree than patients receiving hemodialysis.
Recommendations
The parameter having the most negative impact on the QoL of patients receiving hemodialysis is an impeded possibility to continue work or studies and a change of life plans. That is why, in order to improve their functioning in a manner most similar to healthy persons, the type of renal replacement therapy should consider patients’ individual needs and expectations, ie, guarantee flexible hours of work or study and receiving dialysis.
The will to live was highly assessed by patients receiving peritoneal dialysis as compared to patients receiving hemodialysis. Therefore, the latter group of patients should receive psychological care, in particular those demonstrating emotional problems, in order to achieve better results in therapy and improve their QoL.
In contrast, patients receiving hemodialysis demonstrated numerous eating limitations resulting from the method of treatment, which should prompt the medical personnel to refer such patients to consult a dietitian.
Implications for nursing practice, nursing policy, and health policy and/or social policy
Flexible patient access to dialysis treatment (adjusted to the lifestyle and expectations), especially in patients undergoing hemodialysis.
Constant care clinical psychologist (at every stage of dialysis treatment), also for patients not reporting emotional disorders (prevention of these changes in the future).
Organizing regular training sessions for nurses working in dialysis in clinical psychology and interpersonal communication with the patient.
Hiring a full-time qualified nutritionist in the medical dialysis department to monitor the nutritional status of patients and conduct regular education and nutritional counseling.
Footnotes
Disclosure
The authors report no conflicts of interest with this work.
References
- 1.Heleniak Z, Renke M. Chorzy w podeszłym wieku leczeni hemodializą [Elderly patients treated with peritoneal dialysis] Forum Nefrologiczne. 2009;2(2):97–100. Polish. [Google Scholar]
- 2.Król E, Rutkowski B. Przewlekła choroba nerek – klasyfikacja, epidemiologia, diagnostyka [Chronic kidney disease – classification, epidemiology, diagnostics] Forum Nefrologiczne. 2008;1(1):1–6. Polish. [Google Scholar]
- 3.Nowicki M. Metody wykrywania i oceny postępu przewlekłej choroby nerek [Methods of detection and evaluation of the progress of chronic kidney disease] Choroby Serca i Naczyń. 2007;4(3):137–141. Polish. [Google Scholar]
- 4.Rutkowski B. Przewlekła choroba nerek – wyzwanie XXI wieku [Chronic kidney disease – the challenge of the 21st century] Przewodnik Lekarza. 2007;2:80–88. Polish. [Google Scholar]
- 5.Kiszka W, Załuska W. Społeczny wymiar dializoterapii [Social dimension of dialysis] Zdrowie Publiczne. 2004;114(1):89–92. Polish. [Google Scholar]
- 6.Rutkowski B. Aktualne problemy diagnostyki chorób nerek [Current problems of kidney disease diagnosis] Forum Nefrologiczne. 2009;2(1):45–49. Polish. [Google Scholar]
- 7.Sapilak BJ, Kurpas D, Steciwko A, Melon M. Czy jakość życia jest istotna dla chorych dializowanych? Na podstawie 3-letniej obserwacji pacjentów [Is quality of life important for dialysis patients? Based on 3 years of patient observation] Problemy Lekarskie. 2006;45(3):89–93. Polish. [Google Scholar]
- 8.Dutkowska D, Rumianowski B, Grochans E, Karakiewicz B, Laszczyńska M. Porównanie jakości życia pacjentów hemodi-alizowanych i dializowanych otrzewnowo [Comparison of the life quality of hemodialysis and peritoneal patients] Problemy Higieny i Epidemiologii. 2012;93(3):529–535. Polish. [Google Scholar]
- 9.Kapka-Skrzypczak L, Lipin B, Niedźwiecka J, et al. Subiektywna ocena jakości życia pacjentów dializowanych metodą dializy otrzewnowej oraz hemodializy [Subjective assessment of quality of life of dialysis patients by peritoneal dialysis and hemodialysis] Problemy Higieny i Epidemiologii. 2012;93(4):790–797. Polish. [Google Scholar]
- 10.Ziarko E, Orzeł-Nowak A, Rak A, Libera M, Smoleński O. Jakość życia pacjentów z niewydolnością nerek [Quality of life of patients with renal failure] Pielęgniarka i Położna. 2001;2:4–8. Polish. [Google Scholar]
- 11.Kliś A, Stompór T, Rutkowski B. Jakość życia pacjenta dializowanego [Quality of life of a dialysis patient] In: Rutkowski B, editor. Leczenie nerkozastępcze w praktyce pielęgniarskiej [Renal Replacement Therapy in Nursing Practice] Gdańsk: Via Medica; 2009. Polish. [Google Scholar]
- 12.Stelcer B. Jakość życia jako pojęcie subiektywne i wielowymiarowe [Quality of life as a subjective and multidimensional concept] Pielęgniarstwo Polskie. 2001;2(12):227–232. Polish. [Google Scholar]
- 13.Kłak R, Kaźimierczak K, Penar J, Wende W, Klinger M. Indywidualizacja wyboru metody leczenia nerkozastępczego chorych z nefropatią cukrzycową w oparciu o względy medyczne, psychologiczne i społeczne [Individualization of the choice of renal replacement therapy for patients with diabetic nephropathy based on medical, psychological and social considerations.] Polski Merkuriusz Lekarski. 2005;19(114):835–838. Polish. [PubMed] [Google Scholar]
- 14.Wiśniewska L, Paczkowska B, Białobrzeska B. Zapotrzebowanie na wsparcie emocjonalne wśród pacjentów leczonych nerkozastępczo [Demand for emotional support among patients receiving renal replacement therapy] Forum Nefrologiczne. 2010;3(1):63–70. Polish. [Google Scholar]
- 15.Skowrońska Z. Rola pielęgniarki w wyborze metody leczenia nerkozastępczego [The role of nurse in selection the method of renal replacement therapy] Forum Nefrologiczne. 2012;5(2):170–178. Polish. [Google Scholar]
- 16.Szczegółowe informacje oraz wzory dokumentów [Detailed information and model documents] [Accessed April 5, 2018]. Available from: http://komisja-bioetyczna.wum.edu.pl/content/szczegółowe-informacje-oraz-wzory-dokumentów. Polish.
- 17.Homaie Rad E, Mostafavi H, Delavaris S, Mostafavi S. Health-related quality of life in patients on hemodialysis and peritoneal dialysis: a meta-analysis of Iranian studies. Iran J Kidney Dis. 2015;9(5):386–393. [PubMed] [Google Scholar]
- 18.Mau LW, Chiu HC, Chang PY, Hwang SC, Hwang SJ. Health-related quality of life in Taiwanese dialysis patients: effects of dialysis modality. Kaohsiung J Med Sci. 2008;24(9):453–460. doi: 10.1016/s1607-551x(09)70002-6. [DOI] [PubMed] [Google Scholar]
- 19.Salomão A, Cristelli MP, Santos A. Short daily dialysis’ pilot project: quality of life improvement of chronic renal failure patients. J Bras Nefrol. 2002;24(4):168–175. [Google Scholar]
- 20.Turkmen K, Erdur FM, Guney I, et al. Sleep quality, depression, and quality of life in elderly hemodialysis patients. Int J Nephrol Renovasc Dis. 2012;5:135–142. doi: 10.2147/IJNRD.S36493. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Theofilou P. Quality of life in patients undergoing hemodialysis or peritoneal dialysis treatment. J Clin Med Res. 2011;3(3):132–138. doi: 10.4021/jocmr552w. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Ginieri-Coccossis M, Theofilou P, Synodinou C, Tomaras V, Soldatos C. Quality of life, mental health and health beliefs in hemodialysis and peritoneal dialysis patients: investigating differences in early and later years of current treatment. BMC Nephrol. 2008;9:14. doi: 10.1186/1471-2369-9-14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Gonçalves FA, Dalosso IF, Camargo-Borba JM. Quality of life in chronic renal patients on hemodialysis or peritoneal dialysis: a comparative study in a referral service of Curitiba – PR. J Bras Nefrol. 2015;37(4):467–474. doi: 10.5935/0101-2800.20150074. [DOI] [PubMed] [Google Scholar]
- 24.Sapilak BJ, Kurpas D, Steciwko A, Melon M. Profil osobowości i zaburzenia nastroju pacjentów przewlekle hemodializowanych [Personality profile and mood disorders of chronic hemodialysis patients] Problemy Lekarskie. 2006;45(3):94–96. Polish. [Google Scholar]
- 25.García-Llana H, Remor E, Selgas R. Adherence to treatment, emotional state and quality of life in patients with end-stage renal disease undergoing dialysis. Psicothema. 2013;25(1):79–86. doi: 10.7334/psicothema2012.96. [DOI] [PubMed] [Google Scholar]
- 26.Arenas VG, Barros NFNM, Lemos FB, Martins MA, David-Neto E. Qualidade de vida: comparação entre diálise peritoneal automatizada e hemodiálise. Acta Paul Enferm. 2009;22:535–539. [Google Scholar]
- 27.Fructuoso M, Castro R, Oliveira L, Prata C, Morgado T. Quality of life in chronic kidney disease. Nefrologia. 2011;31(1):91–96. doi: 10.3265/Nefrologia.pre2010.Jul.10483. [DOI] [PubMed] [Google Scholar]
- 28.Misiewicz A, Różański J, Marchelek-Myśliwiec M, Wiśniewska M. Problemy psychospołeczne chorych przewlekle dializowanych [Psychosocial problems of chronic dialysis patients] Postępy Nauk Medycznych. 2010;3:188–191. Polish. [Google Scholar]
- 29.Polaschek N. The experience of living on dialysis: a literature review. Nephrol Nurs J. 2003;30(3):303–309. [PubMed] [Google Scholar]
- 30.Gilbar O, Or-Han K, Plivazky N. Mental adjustment, coping strategies, and psychological distress among end-stage renal disease patients. J Psychosomatic Res. 2005;58(6):471–476. doi: 10.1016/j.jpsychores.2005.01.004. [DOI] [PubMed] [Google Scholar]
- 31.Makara-Studzińska M, Książek P, Koślak A, Załuska Z, Książek A. Roz-powszechnienie zaburzeń depresyjnych wśród pacjentów ze schyłkową niewydolnością nerek [Prevalence of depressive symptoms in patients with end-stage renal disease (ESRD) a review] Psychiatria Polska. 2011;XLV(2):187–195. Polish. [PubMed] [Google Scholar]
- 32.Zhang AH, Cheng LT, Zhu N, Sun LH, Wang T. Comparison of quality of life and causes of hospitalization between hemodialysis and peritoneal dialysis patients in China. Health Qual Life Outcomes. 2007;5:49. doi: 10.1186/1477-7525-5-49. [DOI] [PMC free article] [PubMed] [Google Scholar]