

Abstract
Aims
Both hypo- and hyperkalaemia can have immediate deleterious physiological effects, and less is known about long-term risks. The objective was to determine the risks of all-cause mortality, cardiovascular mortality, and end-stage renal disease associated with potassium levels across the range of kidney function and evaluate for consistency across cohorts in a global consortium.
Methods and results
We performed an individual-level data meta-analysis of 27 international cohorts [10 general population, 7 high cardiovascular risk, and 10 chronic kidney disease (CKD)] in the CKD Prognosis Consortium. We used Cox regression followed by random-effects meta-analysis to assess the relationship between baseline potassium and adverse outcomes, adjusted for demographic and clinical characteristics, overall and across strata of estimated glomerular filtration rate (eGFR) and albuminuria. We included 1 217 986 participants followed up for a mean of 6.9 years. The average age was 55 ± 16 years, average eGFR was 83 ± 23 mL/min/1.73 m2, and 17% had moderate- to-severe increased albuminuria levels. The mean baseline potassium was 4.2 ± 0.4 mmol/L. The risk of serum potassium of >5.5 mmol/L was related to lower eGFR and higher albuminuria. The risk relationship between potassium levels and adverse outcomes was U-shaped, with the lowest risk at serum potassium of 4–4.5 mmol/L. Compared with a reference of 4.2 mmol/L, the adjusted hazard ratio for all-cause mortality was 1.22 [95% confidence interval (CI) 1.15–1.29] at 5.5 mmol/L and 1.49 (95% CI 1.26–1.76) at 3.0 mmol/L. Risks were similar by eGFR, albuminuria, renin–angiotensin–aldosterone system inhibitor use, and across cohorts.
Conclusions
Outpatient potassium levels both above and below the normal range are consistently associated with adverse outcomes, with similar risk relationships across eGFR and albuminuria.
Keywords: Potassium, Estimated glomerular filtration rate, Albuminuria, End-stage renal disease, Mortality
Introduction
Abnormal serum potassium levels represent one of the most important electrolyte disturbances in clinical practice. Potassium plays a crucial role in normal cell membrane electrophysiology, with both hyperkalaemia and hypokalaemia resulting in electrophysiological perturbations, most importantly in the cardiac system. Abnormalities in myocardial resting membrane potential, cardiac depolarization, and myocardial excitability can result in conduction system abnormalities, including malignant arrhythmias.1–3
The kidneys play a central role in potassium homeostasis, with chronic kidney disease (CKD) being an especially prominent risk factor for hyperkalaemia.4,5 Other risk factors for hyperkalaemia commonly occur in combination with CKD, including clinical conditions such as acute kidney injury, cardiovascular disease (CVD), and diabetes mellitus (DM), and various medication classes that affect physiological processes involved in potassium regulation, such as inhibitors of the renin–angiotensin–aldosterone system (RAASi).6 There is wide variation in the estimates of hyperkalaemia incidence and prevalence reported in studies of CKD patients, ranging from as low as 7.7% to as high as 73%.7–10 Although patients in the general population are reported to have lower risk of hyperkalaemia than patients with CKD, with prevalence values ranging from 2.6% to 3.5% in Canadian and US studies, many of these studies are limited by small sample size or select populations.4,10,11 There are less data on hypokalaemia in general. The increasing worldwide prevalence of CKD and associated conditions compels a careful assessment of the prevalence and long-term risks associated with abnormal potassium levels in diverse international populations.12,13
Hyperkalaemia and hypokalaemia have been consistently associated with higher short-term all-cause mortality in observational studies.8,14–18 Some, but not all, have suggested that risks associated with hyperkalaemia are greater in individuals with normal kidney function than in those with CKD.10 Notwithstanding the putative role of cardiac arrhythmias in the mortality associated with hypo- and hyperkalaemia,19 few studies have examined the long-term association of abnormal potassium levels with CVD-associated mortality. Furthermore, the effects of abnormal serum potassium levels on outcomes in other organ systems, such as the kidneys, remain less well studied. To better guide clinical practice and future clinical trials, we performed a meta-analysis of the prevalence of abnormal potassium levels, risk factors of abnormal potassium levels, and long-term associations between potassium levels, all-cause mortality, CVD-associated mortality, and end-stage renal disease (ESRD) in 27 large and diverse international cohorts. For the latter aim, we also evaluated whether risks varied by the level of kidney function and other clinically relevant characteristics.
Methods
Participating cohorts
The Chronic Kidney Disease Prognosis Consortium (CKD-PC) has been described previously; additional information is available in Supplementary material online, AppendicesS1 and S2.20–24 Briefly, CKD-PC incorporates cohorts with at least 1000 participants [at least 500 participants for those cohorts predominantly enrolling persons with CKD [CKD cohorts)], data on serum creatinine and albuminuria, and 50 or more events of the outcome of interest (mortality or kidney outcomes). The present study included 27 cohorts: 10 general population cohorts, 7 high risk cohorts in terms of cardiovascular (CV) risk, and 10 CKD cohorts. Meta-analyses were restricted to participants aged ≥18 years with an available value of potassium at baseline. This study was approved by the institutional review board at the Johns Hopkins Bloomberg School of Public Health (Baltimore, MD, USA).
Procedures
Estimated glomerular filtration rate (eGFR) was calculated using the Chronic Kidney Disease–Epidemiology Collaboration (CKD–EPI) creatinine equation.25 In cohorts where the creatinine measurement was not standardized to isotope dilution mass spectrometry, values were multiplied by 0.95 before eGFR calculation.26 We defined diabetes as fasting glucose ≥7.0 mmol/L (126 mg/dL), non-fasting glucose ≥11.1 mmol/L (200 mg/dL), haemoglobin A1c ≥6.5%, use of glucose-lowering drugs, or self-reported diabetes. Participants with a history of myocardial infarction, coronary revascularization, heart failure, or stroke were considered to have a history of CVD. Measures of albuminuria were the urine albumin-to-creatinine ratio (ACR), urine albumin excretion rate, urine protein-to-creatinine ratio, or semi-quantitative dipstick protein; urine protein-to-creatinine ratio was converted to ACR as previously described.27
The outcomes of interest were all-cause mortality, CVD-associated mortality, and ESRD. We defined ESRD as initiation of renal replacement therapy.
Statistical analysis
We applied a two-stage meta-analysis, with each study first analysed individually, followed by a random-effects meta-analysis. The overview of the analysis and analytic notes for individual studies are provided in Supplementary material, AppendixS2. We imputed missing values of covariates using cohort-specific mean values. Potassium levels, serum creatinine, and albuminuria, as well as the demographic variables age, gender, and race were not imputed. We quantified heterogeneity with the I2 statistic and Cochran’s Q test. Because the risk of abnormal serum potassium levels and their associated outcomes might vary substantially depending on the type of patient population, analyses were stratified by the type of cohort (general population/high CV risk or CKD).
To assess the cross-sectional associations between kidney function and level of potassium, we plotted the distribution of baseline serum potassium levels within categories of eGFR using kernel density plots. Next, we modelled the risk of potassium >5.0, >5.5, and <3.5 mmol/L using logistic regression, adjusting for age, race, gender, systolic blood pressure, antihypertensive drugs, total cholesterol, diabetes mellitus, body mass index, smoking, history of coronary heart disease or stroke, history of heart failure, eGFR (linear spline with knots at 30 and 60), and albuminuria (log-transformed ACR or categories of dipstick). For eGFR and ACR, the reference point was placed at eGFR of 80 mL/min/1.73 m2 and ACR of 10 mg/g in the general population/high CV risk cohorts and eGFR of 50 mL/min/1.73 m2 and ACR of 50 mg/g in the CKD cohorts, with statistical significance at other points determined by the meta-analyzed beta coefficient and standard error. We tested whether the relationship between kidney function and abnormal potassium levels differed by subgroups of age, race, gender, and diabetes status, by including the relevant product term in the regression model, determining statistical significance by evaluating the ratio of odds ratios between subgroups at each 1 mL/min/1.73 m2 and 8% increment of ACR (pointwise interaction), as done previously.20,28,29 In addition, we assessed the relationship between potassium levels >5.5 mmol/L and CKD stages (G1–G5 and A1–A3), with the reference placed as G2/A1 in the general population/high CV risk cohorts and G3b/A2 in the CKD cohorts.
To assess the relationship between baseline serum potassium and subsequent adverse outcomes, we modelled the adjusted hazard ratios (HRs) of the studied outcomes as a spline function of serum potassium concentration, fitting piecewise linear splines for serum potassium with knots placed at 3.5, 4, 4.5, 5, and 5.5 mmol/L, and adjusting for the same set of covariates. Given the importance of kidney function on potassium homeostasis, analyses were performed overall and with interaction between potassium and eGFR strata of 60+, 30–59, and <30 mL/min/1.73 m2; albuminuria levels of <30, 30–299, and ≥300 mg/g as well as age, race, gender, diabetes status, RAASi use, and diuretic use, determining statistical significance for the pointwise interaction at each 0.05 mmol/L of potassium. Analyses were performed using Stata/MP 14.2 software for Windows (www.stata.com). We considered P-values <0.05 as statistically significant.
Results
There were a total of 1 217 986 participants with baseline potassium, eGFR, and albuminuria levels across 27 cohorts, followed up for an average of 6.9 years (range 2.0–19). The average (mean ± standard deviation) age was 55 ± 16 years, 40% were women, and 14% were Black (Table 1). The average eGFR was 83 ± 23 mL/min/1.73 m2, 17% had moderate-to-severe increased albuminuria levels, and 46% were on antihypertensive medications. Angiotensin-converting enzyme inhibitors (ACEi), angiotensin receptor blockers (ARBs), and potassium-sparing diuretics were used in 31%, 11%, and 3% of individuals at baseline, respectively. Non-steroidal anti-inflammatory drugs use was reported by 15% (Supplementary material online, Table S1).
Table 1.
Baseline characteristics
| Study | Region | n | Potassium (mmol/L) | eGFR, (mL/min/ 1.73 m2) | Albuminuria >30 mg/ga | Age (years) | % Female | % Blacks | % DM | % History of CHD and/or stroke | % History of HF | % Current smoker | % HTN | SBP (mmHg) | DBP (mmHg) | BMI (kg/m2) | Chol (mmol/L) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| General population | |||||||||||||||||
| Beijing | China | 1528 | 4.5 (0.5) | 83 (14) | 87 (6%) | 60 (10) | 772 (51%) | 0 (0%) | 420 (29%) | 281 (18%) | — | 360 (24%) | 682 (45%) | 125 (18) | 77 (10) | 25 (3) | 5.3 (1.1) |
| CIRCS | Japan | 8034 | 4.2 (0.4) | 89 (15) | 216 (3%) | 54 (9) | 4990 (62%) | 0 (0%) | 96 (1%) | 88 (1%) | — | 2010 (25%) | 2630 (33%) | 130 (18) | 79 (11) | 23 (3) | 5.1 (0.9) |
| Gubbio | Italy | 1683 | 4.2 (0.4) | 84 (12) | 70 (4%) | 54 (6) | 933 (55%) | 0 (0%) | 90 (5%) | 164 (10%) | 34 (2%) | 524 (31%) | 663 (39%) | 130 (18) | 78 (10) | 28 (4) | 5.9 (1.0) |
| KHS | South Korea | 111532 | 4.2 (0.3) | 86 (15) | 4248 (4%) | 46 (10) | 41692 (37%) | 0 (0%) | 7208 (6%) | 3219 (3%) | — | 38734 (35%) | 29159 (26%) | 122 (18) | 75 (12) | 24 (3) | 5.0 (0.9) |
| MRC | UK | 11840 | 4.4 (0.6) | 57 (15) | 892 (8%) | 81 (5) | 7221 (61%) | 0 (0%) | 917 (8%) | 2058 (18%) | 2 (100%) | 1343 (11%) | 4006 (34%) | 149 (22) | 74 (13) | 26 (4) | — |
| NHANES | USA | 46526 | 4.0 (0.3) | 97 (25) | 5543 (12%) | 47 (20) | 24212 (52%) | 10365 (22%) | 5336 (11%) | 4094 (9%) | 1366 (3%) | 8318 (19%) | 15937 (35%) | 124 (20) | 71 (13) | 28 (6) | 5.2 (1.1) |
| PREVEND | Netherlands | 7319 | 4.4 (0.7) | 96 (16) | 750 (10%) | 50 (13) | 3768 (51%) | 66 (1%) | 263 (4%) | 397 (5%) | 19 (0%) | 2440 (33%) | 2443 (34%) | 129 (20) | 74 (10) | 26 (4) | 5.6 (1.1) |
| Rancho Bernardo | USA | 1481 | 4.3 (0.4) | 66 (16) | 217 (15%) | 71 (12) | 884 (60%) | 1 (0%) | 212 (14%) | 206 (14%) | 50 (3%) | 115 (8%) | 749 (51%) | 135 (22) | 76 (10) | 26 (4) | 5.5 (1.0) |
| Taiwan MJ | Taiwan | 140488 | 4.1 (0.3) | 86 (18) | 3763 (3%) | 44 (15) | 73278 (52%) | 0 (0%) | 8053 (6%) | 5331 (5%) | — | 24904 (26%) | 29211 (21%) | 122 (21) | 74 (12) | 23 (4) | 5.0 (1.0) |
| Takahata | Japan | 1923 | 4.3 (0.4) | 97 (12) | 250 (13%) | 64 (10) | 1064 (55%) | 0 (0%) | 176 (9%) | 131 (7%) | — | 307 (16%) | 1111 (58%) | 134 (16) | 79 (10) | 23 (3) | 5.2 (0.8) |
| Subtotal | 332 354 | 4.1 (0.4) | 87 (19) | 16 036 (5%) | 47 (15) | 158 814 (48%) | 10 432 (19%) | 22 771 (7%) | 15 353 (5%) | 1471 (3%) | 79 055 (28%) | 86 591 (26%) | 124 (21) | 74 (12) | 24 (4) | 5.1 (1.0) | |
| High CV risk cohorts | |||||||||||||||||
| ADVANCE | Multi | 11 003 | 4.4 (0.5) | 78 (17) | 3400 (31%) | 66 (6) | 4681 (43%) | 38 (0%) | 11 003 (100%) | 3099 (28%) | 352 (3%) | — | 9088 (83%) | 145 (21) | 80 (11) | 28 (5) | 5.2 (1.2) |
| Geisinger | USA | 67023 | 4.3 (0.4) | 80 (26) | 23 507 (35%) | 61 (15) | 34798 (52%) | 1600 (2%) | 43 177 (64%) | 17 076 (25%) | 5487 (8%) | 9960 (15%) | 50 350 (75%) | 131 (18) | 75 (11) | 33 (8) | 4.8 (1.1) |
| Maccabi | Israel | 254 379 | 4.4 (0.4) | 86 (21) | 40 885 (16%) | 58 (14) | 125 220 (49%) | 0 | 90 676 (36%) | 38 332 (15%) | 5989 (2%) | 5695 (2%) | 140 464 (55%) | 131 (18) | 78 (10) | 30 (12) | 4.9 (1.1) |
| Mt Sinai BioMe | USA | 8393 | 4.3 (0.6) | 73 (28) | 2043 (24%) | 56 (14) | 4810 (57%) | 2773 (33%) | 4244 (51%) | 830 (10%) | 1000 (12%) | 1374 (18%) | 6156 (73%) | 132 (20) | 77 (12) | 31 (8) | 4.8 (1.2) |
| RCAV | USA | 277 226 | 4.3 (0.4) | 77 (17) | 746 27 (27%) | 64 (11) | 9213 (3%) | 45 078 (16%) | 218 374 (79%) | 93 440 (34%) | 18 581 (7%) | — | 225 997 (82%) | 133 (17) | 75 (11) | 32 (6) | 4.4 (1.1) |
| SCREAM | Sweden | 224 285 | 4.1 (0.4) | 91 (24) | 24 005 (11%) | 49 (17) | 123 720 (55%) | 0 | 29 690 (13%) | 23 711 (11%) | 12 300 (5%) | — | 49 250 (22%) | — | — | — | 5.2 (1.1) |
| ZODIAC | Netherlands | 1153 | 4.4 (0.4) | 68 (17) | 92 (8%) | 67 (12) | 632 (55%) | 0 | 1153 (100%) | 408 (35%) | — | 217 (19%) | 876 (76%) | 152 (24) | 83 (11) | 29 (5) | 5.5 (1.1) |
| Subtotal | 843 462 | 4.3 (0.4) | 84 (22) | 168 559 (20%) | 58 (15) | 303 074 (36%) | 49 489 (14%) | 408 469 (48%) | 176 233 (21%) | 43 709 (5%) | 17 246 (5%) | 543 172 (64%) | 132 (18) | 76 (11) | 31 (9) | 4.8 (1.2) | |
| CKD cohorts | |||||||||||||||||
| AASK | USA | 1081 | 4.2 (0.6) | 46 (16) | 591 (55%) | 55 (11) | 420 (39%) | 1081 (100%) | 0 | 535 (49%) | 32 (3%) | 317 (29%) | 1081 (100%) | 143 (22) | 88 (14) | 31 (7) | 5.5 (1.2) |
| BC CKD | Canada | 11 990 | 4.6 (0.6) | 34 (17) | 8660 (72%) | 69 (14) | 5473 (46%) | 50 (0%) | 7315 (61%) | 3592 (30%) | 1564 (13%) | 635 (11%) | 10 149 (85%) | 137 (23) | 73 (13) | 28 (6) | 4.6 (1.3) |
| CanPREDDICT | Canada | 2017 | 4.6 (0.6) | 27 (9) | 1487 (74%) | 68 (13) | 755 (37%) | 32 (2%) | 1010 (50%) | 640 (32%) | 269 (13%) | — | 1973 (98%) | 134 (20) | 71 (12) | 30 (8) | 4.2 (1.2) |
| CKD-JAC | Japan | 2639 | 4.6 (0.6) | 37 (17) | 2335 (88%) | 60 (11) | 1001 (38%) | 0 | 896 (34%) | 407 (15%) | 104 (4%) | 385 (17%) | 2472 (94%) | 132 (19) | 76 (12) | 23 (4) | 5.0 (1.1) |
| CRIB | UK | 373 | 4.6 (0.6) | 22 (11) | 314 (84%) | 62 (14) | 130 (35%) | 20 (5%) | 64 (17%) | 93 (25%) | — | 47 (13%) | 350 (94%) | 152 (22) | 84 (12) | 27 (5) | 5.6 (1.3) |
| MASTERPLAN | Netherlands | 670 | 4.4 (0.6) | 36 (15) | 483 (72%) | 60 (13) | 207 (31%) | 0 | 163 (24%) | 171 (26%) | 108 (17%) | 138 (21%) | 639 (95%) | 139 (21) | 80 (12) | 27 (5) | 4.8 (1.1) |
| MDRD | USA | 832 | 4.4 (0.6) | 33 (14) | 619 (74%) | 52 (12) | 329 (40%) | 64 (8%) | 82 (10%) | 90 (11%) | — | 81 (10%) | 724 (87%) | 131 (19) | 80 (10) | 27 (4) | 5.5 (1.3) |
| PSP-CKD | UK | 16 828 | 4.6 (0.5) | 51 (14) | 5364 (32%) | 76 (11) | 10 138 (60%) | 179 (1%) | 5129 (30%) | 5685 (34%) | 1262 (7%) | 1567 (14%) | 16 271 (97%) | 134 (16) | 74 (10) | 29 (6) | 4.4 (1.2) |
| SRR-CKD | Sweden | 2618 | 4.4 (0.6) | 24 (11) | 2061 (79%) | 68 (14) | 844 (32%) | 0 | 990 (38%) | 399 (15%) | 379 (14%) | — | 2526 (97%) | 141 (23) | 78 (12) | 28 (5) | 5.0 (1.5) |
| Sunnybrook | Canada | 3122 | 4.4 (0.5) | 56 (31) | 2167 (69%) | 61 (18) | 1443 (46%) | 0 | 1467 (47%) | 244 (8%) | 217 (7%) | 414 (13%) | 2397 (77%) | 133 (20) | 76 (12) | 29 (12) | 4.8 (1.4) |
| Subtotal | 42 170 | 4.6 (0.6) | 42 (19) | 24 081 (57%) | 70 (14) | 20 740 (49%) | 1426 (4%) | 17 116 (42%) | 11 856 (28%) | 3935 (10%) | 3584 (14%) | 38 582 (91%) | 135 (20) | 75 (12) | 28 (7) | 4.6 (1.3) | |
| Total | 1 217 986 | 4.2 (0.4) | 83 (23) | 208 676 (17%) | 55 (16) | 482 628 (40%) | 61 347 (14%) | 448 356 (37%) | 203 442 (17%) | 49 115 (5%) | 99 885 (16%) | 66 8345 (55%) | 129 (19) | 76 (11) | 29 (9) | 4.9 (1.1) | |
CHD, coronary heart disease; CVD, cardiovascular disease; DBP, diastolic blood pressure; DM, diabetes mellitus; eGFR, estimated glomerular filtration rate; HF, heart failure; HTN, hypertension; SBP, systolic blood pressure.
By definition, all participants have a measure of albuminuria. Urine protein-to-creatinine ratio was converted to urine albumin-to-creatinine ratio by dividing by 2.655 for men and 1.7566 for women. Dipstick proteinuria was classified as <30 mg/g for values of negative and trace, 30–299 mg/g for 1+, and 300+ mg/g for 2+ and higher.
Prevalence and risk factors of hyperkalaemia and hypokalaemia
Overall, the average baseline potassium was 4.2 ± 0.4 mmol/L; potassium was higher with lower baseline eGFR in both the general population/high CV risk cohorts (Figure 1) and the CKD cohorts (Supplementary material online, Figure S1). The prevalence of serum potassium >5.0 mmol/L, serum potassium >5.5 mmol/L, serum potassium <4.0 mmol/L, and serum potassium <3.5 mmol/L was 3.31% [95% confidence interval (CI) 3.28–3.34%], 0.49% (95% CI 0.48–0.50%), 23.57% (95% CI 23.49–23.64%), and 1.91% (95% CI 1.89–1.94%) of individuals in general population/high CV risk cohorts and 17.94% (95% CI 17.58–18.31%), 4.23% (95% CI 4.03–4.42%), 12.61% (95% CI 12.29–12.93%), and 2.03% (95% CI 1.90–2.17%) of individuals in the CKD cohorts. In the general population/high CV risk cohorts, risk factors for hyperkalaemia included male gender, non-Black race, DM, lower body mass index (BMI), active smoking, history of coronary heart disease or stroke, lower eGFR, higher ACR, use of ACEi, ARB, or potassium-sparing diuretics, and non-use of thiazide or loop diuretics (Supplementary material online, Table S2). The relationship between eGFR and serum potassium >5.5 mmol/L was nearly linear; higher ACR was a weaker but an independent risk factor at levels >37 mg/g (Figure 2A and B). There were no meaningful differences in the relationship between eGFR or ACR and potassium levels >5.5 mmol/L among patients with different age (<65 years and ≥65 years), gender, race (Black and non-Black), and presence/absence of DM (Supplementary material online, Figures S2). Relationships between eGFR, ACR, and potassium >5.5 mmol/L were also similar in the CKD cohorts (Supplementary material online, Figure S6), as were the direction of associations with most risk factors (Supplementary material online, Table S3). Categorical analysis revealed that lower eGFR was associated with higher risk of potassium level >5.5 mmol/L independent of ACR levels, whereas the association between ACR and hyperkalaemia was most apparent at higher levels of eGFR and null at eGFR <15 mL/min/1.73 m2 (Supplementary material online, Table S4). Similarly, in the CKD cohorts, lower eGFR was a strong risk factor for potassium >5.5 mmol/L, whereas higher ACR was weak to null (Supplementary material online, Table S5).
Figure 1.

Distribution of serum potassium concentrations, overall and by baseline estimated glomerular filtration rate in the general population and high cardiovascular risk cohorts.
Figure 2.

Continuous association of estimated glomerular filtration rate (A) and albuminuria (B) with the risk of serum potassium level >5.5 mmol/L and of estimated glomerular filtration rate (C) and albuminuria (D) with the risk of serum potassium level <3.5 mmol/L, in the general population and high cardiovascular risk cohorts. Black dots indicate statistical significance compared with the reference (diamond) estimated glomerular filtration rate of 80 mL/min/1.73 m2 (A and C) and albuminuria of 10 mg/g (B and D). Adjusted for age, gender, race, systolic blood pressure, antihypertensive drugs, total cholesterol, diabetes, body mass index, smoking, history of coronary heart disease or stroke, and history of heart failure.
Risk factors for hypokalaemia in the general population/high CV risk cohorts included younger age, female gender, Black race, higher systolic blood pressure, the use of thiazide or loop diuretics, lower serum cholesterol, lower BMI, and higher ACR; the use of ACEi, ARB, or potassium-sparing diuretics; the presence of DM; and a history of CHD or stroke were protective (Supplementary material online, Table S2). The association of higher albuminuria level with the risk of hypokalaemia was weak but nearly linear; the association between eGFR and potassium <3.5 mmol/L was fairly flat (Figure 2). Risk factor associations with potassium <3.5 mmol/L were generally consistent in direction if weaker in the CKD cohorts, with the exception of the use of RAASi medications, which was a stronger protective factor for hypokalaemia <3.5 mmol/L in the CKD cohorts (Supplementary material online, Table S3). Neither eGFR nor ACR were significantly associated with potassium <3.5 mmol/L in the CKD cohorts (Supplementary material online, Figure S6).
Outcomes associated with serum potassium level
We observed a total of 151 153 all-cause deaths in 26 cohorts, 9672 CV deaths in 13 cohorts, and 14 266 ESRD events in 16 cohorts during a mean follow-up period of 6.9 ± 4.1 years (Supplementary material online, Table S6). The risk relationship between potassium and all-cause mortality demonstrated lowest risk with serum potassium levels between 4 mmol/L and 4.5 mmol/L and higher risk outside of the 3.5–5 mmol/L range (Figure 3A). Compared with a reference of 4.2 mmol/L, the overall adjusted HR for all-cause mortality was 1.22 (95% CI 1.15–1.29) at serum potassium 5.5 mmol/L and 1.49 (95% CI 1.26–1.76) at serum potassium 3.0 mmol/L. These associations were qualitatively consistent in the individual cohorts (Figure 4), and there was no difference in the risk of all-cause mortality associated with potassium by level of eGFR (Figure 3B). Risk relationships were similarly U-shaped for CV mortality and end-stage renal disease (Figure 3C and D) with qualitative consistency in point estimates (Supplementary material online, , Figures S7 and S8). Although confidence intervals were wide, there appeared to be no difference in potassium–CV risk relationships by the level of eGFR (Supplementary material online, Figure S9A). In contrast, higher levels of potassium had a weaker relationship with ESRD in individuals with eGFR <30 mL/min/1.73 m2 (Supplementary material online, Figure S9B). The associations of serum potassium with the studied outcomes were broadly similar in individuals of different gender, race, levels of albuminuria, history of DM, and ACEi/ARB/potassium-sparing diuretic use; however, the association between lower levels of potassium and all-cause mortality appeared slightly weaker in older individuals and those using diuretics (Supplementary material online, Figures S10–S16). Results were also broadly similar in the CKD cohorts (Supplementary material online, Figures S17–S25).
Figure 3.

Adjusted hazard ratio of all-cause mortality, cardiovascular mortality, and end-stage renal disease associated with serum potassium concentration in the general population and high cardiovascular risk cohorts. Black dots indicate statistical significance compared with the reference (diamond) serum potassium of 4.2 mmol/L. Models adjusted for age, gender, race, systolic blood pressure, antihypertensive drugs, total cholesterol, diabetes, body mass index, smoking, estimated glomerular filtration rate, albuminuria, history of coronary heart disease or stroke, and history of heart failure.
Figure 4.
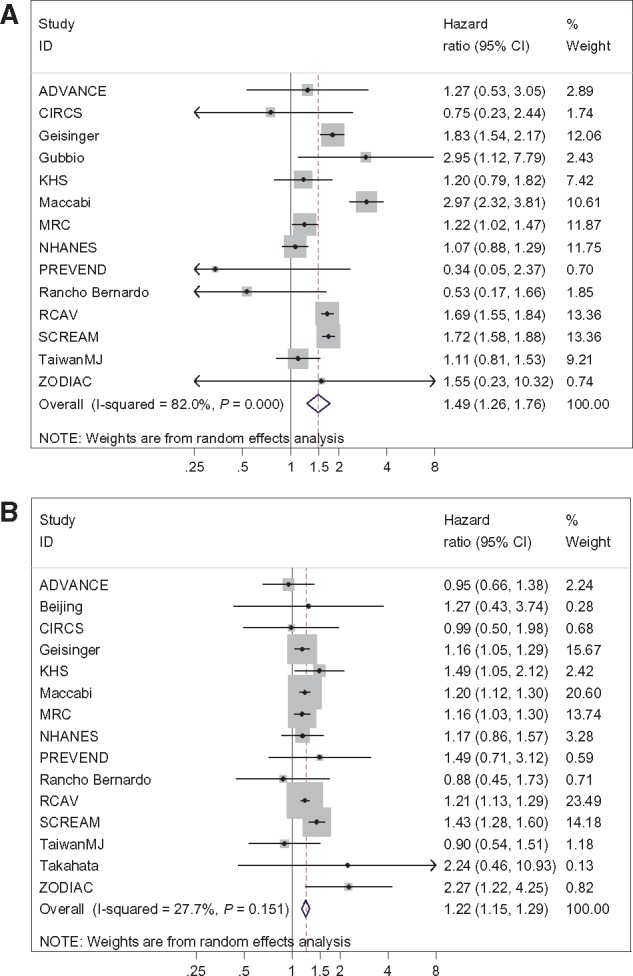
Adjusted relative hazard of all-cause mortality for potassium of 3.0 mmol/L (A) and 5.5 mmol/L (B) compared with a potassium of 4.2 mmol/L in individual general population/high cardiovascular risk cohorts.
Discussion
In this international meta-analysis of 1 217 986 participants in 27 diverse cohorts, we describe the prevalence, risk factors, and long-term outcomes associated with abnormal potassium concentrations. Hyperkalaemia and hypokalaemia were relatively infrequent in the studied populations, especially in participants with normal kidney function. Lower eGFR was a strong risk factor for hyperkalaemia but not hypokalaemia; higher albuminuria was a relatively weak risk factor for both. Both hyper- and hypokalaemia were associated with significantly higher long-term risk of all-cause and CV mortality, and of ESRD. Ideal outcomes were observed with serum potassium concentrations of 4–4.5 mmol/L. While abnormal potassium levels were more common in individuals with lower estimated GFR and higher albuminuria levels, the relative risks associated with hyperkalaemia and hypokalaemia were similar in patients with various levels of kidney function and in various subgroups divided by age, gender, race, DM, or treatment with ACEi or ARB.
Abnormal potassium homeostasis is more frequently mediated by a combination of conditions affecting potassium intake, distribution and excretion, including demographic characteristics, co-morbidities, and various medications.6,30 Our results confirm the diversity of the risk factors determining hyper- and hypokalaemia [including co-morbidities such as congestive heart failure (CHF) and DM,3 and therapeutic interventions such as diuretic use and RAASi31] and emphasize the central role played by the kidneys in potassium homeostasis. Similar to our findings, previous studies have found a low prevalence of hyperkalaemia in patients with normal kidney function and markedly elevated frequencies in various cohorts with CKD, especially in patients with DM, in those with more advanced stages of CKD7,8,10 and in kidney transplant recipients.9 As opposed to the widely accepted role of lower eGFR as a risk factor for hyperkalaemia, the role of albuminuria in engendering this condition has not been previously studied. Our results suggest that patients with higher levels of albuminuria had a higher prevalence of both hyperkalaemia and hypokalaemia, although the magnitude of this association was smaller than the relationship between eGFR and potassium abnormalities, at least for hyperkalaemia. This finding has important practical relevance, because patients with higher levels of albuminuria often benefit from therapy with RAASi medications to slow progression of CKD,32–37 which also increase the risk of hyperkalaemia.31,38,39 A secondary analysis of the Reduction of Endpoints in NIDDM with the Angiotensin II Antagonist Losartan (RENAAL) study showed that hyperkalaemia after losartan therapy attenuated the renoprotective effect of losartan, suggesting that prevention of hyperkalaemia might allow for enhanced renoprotection by RAASi.40 Current clinical guidelines recommend concerted efforts to resume RAASi therapy in patients with CHF, even after episodes of severe hyperkalaemia (>6 mEq/l), once hyperkalaemia was treated and precautions are taken to monitor serum potassium.31 Recent clinical trials suggest that the use of potassium binder medications may allow the use of RAASi in patients prone to hyperkalaemia,41–45 although the long-term benefit of such strategies on clinical outcomes is yet to be demonstrated.46
Although the prevalence of serum potassium <3.5 mmol/L was relatively low, milder forms of hypokalaemia were very common, especially in the general population/high CV risk cohorts. Even mild hypokalaemic episodes are clinically relevant in patients at high risk for ventricular arrhythmias and sudden cardiac death, such as patients with CHF or DM.3,31,47 Correction of hypokalaemia is relatively easy with dietary or medicinal measures,48 and it is recommended as part of strategies to prevent these complications.3
The U-shaped association of serum potassium levels with clinical outcomes described in this study confirms the findings from previous studies, indicating similar associations with all-cause mortality,8,10,14–18 and extends them to an outpatient, large and diverse international population. The association between hypo- and hyperkalaemia and mortality could be explained by the induction of malignant arrhythmias3,19 and their consequences, such as hypotension, myocardial ischaemia, and sudden cardiac death.3,17 In addition, hypokalaemia and low dietary potassium intake are also associated with hypertension and consequent CV outcomes such as strokes.48 This hypothesis is also supported by the association of hypo- and hyperkalaemia with CV mortality in our study. It is perhaps not surprising to see an association of serum potassium levels with ESRD, which has been inconsistently detected previously in smaller cohort studies.8,40,49,50 Hyperkalaemia that is resistant to treatment is an indication of dialysis start, and patients who require very high diuretic doses due to volume overload may have lower potassium levels and may be started earlier on dialysis. In addition to its link with hypertension, hypokalaemia is also a risk factor for tubulointerstitial fibrosis and renal cyst formation,51–54 thus contributing to the development and progression of CKD. Conversely, hyperkalaemia may be a surrogate marker of more severe CKD. Further studies are needed to determine whether correction of hypo- and hyperkalaemia could result in improved renal outcomes.
Our study is notable for its large size, international representation, and diverse patient population. Despite its advantages, this study also has limitations. Variation in design across cohorts introduces heterogeneity and prevents using time-updated potassium levels, but our consistent results across diverse cohorts suggest the robust and empirical long-term association of a single measurement, relevant to clinical practice. Our results were driven largely by findings from general population cohorts, with high CV risk and CKD cohorts contributing relatively fewer participants. However, the causes and consequences of abnormal serum potassium have been least studied in the general population, hence our emphasis on this segment fills an important void. We adjusted for many confounders, but the effect of unmeasured confounders (e.g. serum calcium, magnesium, and blood pH levels) cannot be ruled out. We could not limit the studied medications (e.g. RAASi) to new prescriptions, which may explain their lack of association with outcomes.
Conclusions
The risk factors of abnormal potassium values are diverse and include low estimated GFR, albuminuria, the use of various medications and co-morbid conditions such as DM. The incorporation of these findings in clinical prediction tools in future studies could enhance our ability to risk stratify patients and to proactively manage hypo- and hyperkalaemia. Hypo- and hyperkalaemia are independently associated with significantly higher all-cause and CV mortality, and with higher risk of ESRD, with the best outcomes seen with serum potassium levels of 4–4.5 mmol/L. Future research is needed, preferably in the form of a randomized controlled clinical trial to determine whether the correction of abnormal serum potassium levels can result in improvement in mortality and delayed onset of dialysis.
Authors’ contributions
C.P.K., K.M., J.C., S.H., V.S., and M.E.G. conceived of the study concept and design. K.M., J.C., M.E.G. and the CKD-PC Investigators/Collaborators listed below acquired the data. Y.S. and the Data Coordinating Center members listed below analysed the data. All authors took part in the interpretation of the data. C.P.K., K.M., Y.S., and M.E.G. drafted the manuscript, and all authors provided critical revisions of the manuscript for important intellectual content. All collaborators shared data and were given the opportunity to comment on the manuscript. J.C. obtained funding for CKD-PC and individual cohort and collaborator support is listed in Supplementary material online, AppendixS3.
Supplementary material
Supplementary material is available at European Heart Journal online.
Supplementary Material
Acknowledgements
CKD-PC Investigators/Collaborators (study acronyms/abbreviations provided in italics are listed in Supplementary material online, Appendix S2): AASK: Brad Astor, Larry Appel, Tom Greene, Teresa Chen; ADVANCE: John Chalmers, Mark Woodward, Hisatomi Arima, Vlado Perkovic; BC CKD: Adeera Levin, Ognjenka Djurdjev; Beijing: Luxia Zhang, Lisheng Liu, Minghui Zhao, Fang Wang, Jinwei Wang; CanPREDDICT: Adeera Levin, Ognjenka Djurdjev, Mila Tang; CIRCS: Hiroyasu Iso, Kazumasa Yamagishi, Mitsumasa Umesawa, Isao Muraki; CKD-JAC: Masafumi Fukagawa, Shoichi Maruyama, Takayuki Hamano, Takeshi Hasegawa, Naohiko Fujii; CRIB: David Wheeler, John Emberson, John Townend, Martin Landray; Geisinger: Jamie Green, H. Lester Kirchner, Alex R. Chang; Gubbio: Massimo Cirillo; KHS: Sun Ha Jee, Heejin Kimm, Yejin Mok; Maccabi: Gabriel Chodick, Varda Shalev; MASTERPLAN: Jack F.M. Wetzels, Peter J. Blankestijn, Arjan D. van Zuilen, M. Bots; MDRD: Mark Sarnak, Lesley Inker; MRC: Dorothea Nitsch, Paul Roderick, Astrid Fletcher; Mt Sinai BioMe: Erwin Bottinger, Girish N Nadkarni, Stephen B Ellis, Rajiv Nadukuru; NHANES: Yingying Sang; PSP-CKD: Nigel Brunskill, Rupert Major, David Shepherd, James Medcalf; PREVEND: Ron T Gansevoort, Stephan J.L. Bakker, Hiddo J. Lambers Heerspink; Rancho Bernardo: Simerjot K. Jassal, Jaclyn Bergstrom, Joachim H. Ix, Elizabeth Barrett-Connor; RCAV: Csaba Kovesdy, Kamyar Kalantar-Zadeh; RENAAL: Hiddo J. Lambers Heerspink, Dick de Zeeuw, Barry Brenner; SCREAM: Juan J. Carrero, Alessandro Gasparini, Carl-Gustaf Elinder, Peter Barany; SRR-CKD: Marie Evans, Mårten Segelmark, Maria Stendahl, Staffan Schön; Sunnybrook: Navdeep Tangri, Maneesh Sud, David Naimark; Taiwan MJ: Chi-Pang Wen, Chwen-Keng Tsao, Min-Kugng Tsai, Chien-Hua Chen; Takahata: Tsuneo Konta, Atsushi Hirayama, Kazunobu Ichikawa; ZODIAC: Henk J.G. Bilo, Gijs W.D. Landman, Kornelis J.J. van Hateren, Nanne Kleefstra. CKD-PC Steering Committee: Josef Coresh (Chair), Ron T. Gansevoort, Morgan E. Grams, Stein Hallan, Csaba P. Kovesdy, Andrew S. Levey, Kunihiro Matsushita, Varda Shalev, Mark Woodward. CKD-PC Data Coordinating Center: Shoshana H. Ballew (Assistant Project Director), Jingsha Chen (Programmer), Josef Coresh (Principal Investigator), Morgan E. Grams (Director of Nephrology Initiatives), Lucia Kwak (Programmer), Kunihiro Matsushita (Director), Yingying Sang (Lead Programmer), Mark Woodward (Senior Statistician). Some of the data reported here have been supplied by the United States Renal Data System (USRDS). The interpretation and reporting of these data are the responsibility of the authors and in no way should be seen as an official policy or interpretation of the US government.
Funding
The CKD-PC Data Coordinating Center is funded in part by a programme grant from the US National Kidney Foundation (NKF funding sources include Relypsa) and the National Institute of Diabetes and Digestive and Kidney Diseases (R01DK100446-01). A variety of sources have supported enrolment and data collection including laboratory measurements and follow-up in the collaborating cohorts of the CKD-PC. These funding sources include government agencies such as national institutes of health and medical research councils as well as foundations and industry sponsors listed in Supplementary material online, Appendix S3. The funders had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Conflict of interest: C.P.K. reports grants from National Institutes of Health (NIH), during the conduct of the study; personal fees from Astra Zeneca, personal fees from Relypsa, personal fees from ZS Pharma outside the submitted work. K.M. reports grants and personal fees from Kyowa Hakko Kirin outside the submitted work. N.J.B. reports grants from the UK National Institute for Health Research during the conduct of the study; grants from Baxter Healthcare outside the submitted work. J.J.C. reports grants from AstraZeneca and grants from ViforPharma outside the submitted work. T.H. reports grants from JSPS KAKENHI and personal fees from Kyowa Hakko Kirin outside the submitted work. H.L.H. reports other support from Abbvie, grants and other support from AstraZeneca, other support from Astellas, grants and other support from Boehringer Ingelheim, grants and other support from Janssen, other support from Fresenius, and other support from Merck outside the submitted work. D.C.W. reports grants and personal fees from AstraZeneca, and personal fees from Vifor Fresenius outside the submitted work. J.C. reports grants from NIH and grants from NKF during the conduct of the study; grants from NIH and grants from NKF outside the submitted work; In addition, J.C. has a patent PCT/US2015/044567 Provisional patent [Coresh, Inker and Levey] filed 8/15/2014—precise estimation of glomerular filtration rate from multiple biomarkers issued. Y.S., G.C., A.H., G.W.D.L., A.L., D.N., S.I.H., V.S., and M.E.G. have nothing to disclose.
Footnotes
See page 1543 for the editorial comment on this article (doi: 10.1093/eurheartj/ehy159)
Contributor Information
CKD Prognosis Consortium:
Brad Astor, Larry Appel, Tom Greene, Teresa Chen, John Chalmers, Mark Woodward, Hisatomi Arima, Vlado Perkovic, Adeera Levin, Ognjenka Djurdjev, Luxia Zhang, Lisheng Liu, Minghui Zhao, Fang Wang, Jinwei Wang, Adeera Levin, Ognjenka Djurdjev, Mila Tang, Hiroyasu Iso, Kazumasa Yamagishi, Mitsumasa Umesawa, Isao Muraki, Masafumi Fukagawa, Shoichi Maruyama, Takayuki Hamano, Takeshi Hasegawa, Naohiko Fujii, David Wheeler, John Emberson, John Townend, Martin Landray, Jamie Green, H Lester Kirchner, Alex R Chang, Massimo Cirillo, Sun Ha Jee, Heejin Kimm, Yejin Mok, Gabriel Chodick, Varda Shalev, Jack F M Wetzels, Peter J Blankestijn, Arjan D van Zuilen, M Bots, Mark Sarnak, Lesley Inker, Dorothea Nitsch, Paul Roderick, Astrid Fletcher, Erwin Bottinger, Girish N Nadkarni, Stephen B Ellis, Rajiv Nadukuru, Yingying Sang, Nigel Brunskill, Rupert Major, David Shepherd, James Medcalf, Ron T Gansevoort, Stephan J L Bakker, Hiddo J Lambers Heerspink, Simerjot K Jassal, Jaclyn Bergstrom, Joachim H Ix, Elizabeth Barrett-Connor, Csaba Kovesdy, Kamyar Kalantar-Zadeh, Hiddo J Lambers Heerspink, Dick de Zeeuw, Barry Brenner, Juan J Carrero, Alessandro Gasparini, Carl-Gustaf Elinder, Peter Barany, Marie Evans, Mårten Segelmark, Maria Stendahl, Staffan Schön, Navdeep Tangri, Maneesh Sud, David Naimark, Chi-Pang Wen, Chwen-Keng Tsao, Min-Kugng Tsai, Chien-Hua Chen, Tsuneo Konta, Atsushi Hirayama, Kazunobu Ichikawa, Henk J G Bilo, Gijs W D Landman, Kornelis J J van Hateren, Nanne Kleefstra, Josef Coresh, Ron T Gansevoort, Morgan E Grams, Stein Hallan, Csaba P Kovesdy, Andrew S Levey, Kunihiro Matsushita, Varda Shalev, Mark Woodward, Shoshana H Ballew, Jingsha Chen, Josef Coresh, Morgan E Grams, Lucia Kwak, Kunihiro Matsushita, Yingying Sang, and Mark Woodward
References
- 1. Dittrich KL, Walls RM.. Hyperkalemia: eCG manifestations and clinical considerations. J Emerg Med 1986;4:449–455. [DOI] [PubMed] [Google Scholar]
- 2. Parham WA, Mehdirad AA, Biermann KM, Fredman CS.. Hyperkalemia revisited. Tex Heart Inst J 2006;33:40–47. [PMC free article] [PubMed] [Google Scholar]
- 3. Priori SG, Blomstrom-Lundqvist C.. 2015 European Society of Cardiology Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death summarized by co-chairs. Eur Heart J 2015;36:2757–2759. [DOI] [PubMed] [Google Scholar]
- 4. Drawz PE, Babineau DC, Rahman M.. Metabolic complications in elderly adults with chronic kidney disease. J Am Geriatr Soc 2012;60:310–315. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Bourgoignie JJ, Kaplan M, Pincus J, Gavellas G, Rabinovitch A.. Renal handling of potassium in dogs with chronic renal insufficiency. Kidney Int 1981;20:482–490. [DOI] [PubMed] [Google Scholar]
- 6. Kovesdy CP. Management of hyperkalaemia in chronic kidney disease. Nat Rev Nephrol 2014;10:653–662. [DOI] [PubMed] [Google Scholar]
- 7. Sarafidis PA, Blacklock R, Wood E, Rumjon A, Simmonds S, Fletcher-Rogers J, Ariyanayagam R, Al-Yassin A, Sharpe C, Vinen K.. Prevalence and factors associated with hyperkalemia in predialysis patients followed in a low-clearance clinic. Clin J Am Soc Nephrol 2012;7:1234–1241. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Hayes J, Kalantar-Zadeh K, Lu JL, Turban S, Anderson JE, Kovesdy CP.. Association of hypo- and hyperkalemia with disease progression and mortality in males with chronic kidney disease: the role of race. Nephron Clin Pract 2012;120:c8–16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Palmer BF. Managing hyperkalemia caused by inhibitors of the renin-angiotensin-aldosterone system. N Engl J Med 2004;351:585–592. [DOI] [PubMed] [Google Scholar]
- 10. Einhorn LM, Zhan M, Hsu VD, Walker LD, Moen MF, Seliger SL, Weir MR, Fink JC.. The frequency of hyperkalemia and its significance in chronic kidney disease. Arch Intern Med 2009;169:1156–1162. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Fleet JL, Shariff SZ, Gandhi S, Weir MA, Jain AK, Garg AX.. Validity of the International Classification of Diseases 10th revision code for hyperkalaemia in elderly patients at presentation to an emergency department and at hospital admission. BMJ Open 2012;2:e002011.. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Coresh J, Selvin E, Stevens LA, Manzi J, Kusek JW, Eggers P, Van Lente F, Levey AS.. Prevalence of chronic kidney disease in the United States. JAMA 2007;298:2038–2047. [DOI] [PubMed] [Google Scholar]
- 13. Mills KT, Xu Y, Zhang W, Bundy JD, Chen CS, Kelly TN, Chen J, He J.. A systematic analysis of worldwide population-based data on the global burden of chronic kidney disease in 2010. Kidney Int 2015;88:950–957. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Lowrie EG, Lew NL.. Death risk in hemodialysis patients: the predictive value of commonly measured variables and an evaluation of death rate differences between facilities. Am J Kidney Dis 1990;15:458–482. [DOI] [PubMed] [Google Scholar]
- 15. Iseki K, Uehara H, Nishime K, Tokuyama K, Yoshihara K, Kinjo K, Shiohira Y, Fukiyama K.. Impact of the initial levels of laboratory variables on survival in chronic dialysis patients. Am J Kidney Dis 1996;28:541–548. [DOI] [PubMed] [Google Scholar]
- 16. Kovesdy CP, Regidor DL, Mehrotra R, Jing J, McAllister CJ, Greenland S, Kopple JD, Kalantar-Zadeh K.. Serum and dialysate potassium concentrations and survival in hemodialysis patients. Clin J Am Soc Nephrol 2007;2:999–1007. [DOI] [PubMed] [Google Scholar]
- 17. Goyal A, Spertus JA, Gosch K, Venkitachalam L, Jones PG, Van den Berghe G, Kosiborod M.. Serum potassium levels and mortality in acute myocardial infarction. Jama 2012;307:157–164. [DOI] [PubMed] [Google Scholar]
- 18. Korgaonkar S, Tilea A, Gillespie BW, Kiser M, Eisele G, Finkelstein F, Kotanko P, Pitt B, Saran R.. Serum potassium and outcomes in CKD: insights from the RRI-CKD cohort study. Clin J Am Soc Nephrol 2010;5:762–769. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Epstein FH, Signs and symptoms of electrolyte disorders In: Maxwell MH, Kleeman CR (eds). Clinical Disorders of Fluid and Electrolyte Metabolism. 3rd ed.New York: McGraw-Hill; 1980. p499–516. [Google Scholar]
- 20. Grams ME, Sang Y, Ballew SH, Gansevoort RT, Kimm H, Kovesdy CP, Naimark D, Oien C, Smith DH, Coresh J, Sarnak MJ, Stengel B, Tonelli M, Tonelli M, Hemmelgarn BR, James MT, Turin TC, Coresh J, Matsushita K, Grams M, Sang Y, Shlipak M, Sarnak MJ, Katz R, Wheeler DC, Emberson J, Landray MJ, Townend JN, Green J, Kirchner HL, Perkins R, Chang AR, Romundstad S, Aasarød K, Øien CM, Hallan S, Smith DH, Thorp ML, Johnson ES, Chodick G, Herzel E, Katz R, Shalev V, Gansevoort RT, Bakker SJL, Lambers Heerspink HJ, van der Harst P, Jee SH, Kimm H, Mok Y, Tangri N, Naimark D, Ärnlöv J, Larsson A, Lannfelt L, Kovesdy CP, Kalantar-Zadeh K, Coresh J, Grams M, Matsushita K, Gansevoort RT, de Jong PE, Iseki K, Levey AS, Sarnak MJ, Stengel B, Warnock D, Woodward M, Ballew SH, Coresh J, Grams M, Matsushita K, Sang Y, Woodward M.. A meta-analysis of the association of estimated GFR, albuminuria, age, race, and sex with acute kidney injury. Am J Kidney Dis 2015;66:591–601. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Grams ME, Sang Y, Levey AS, Matsushita K, Ballew S, Chang AR, Chow EK, Kasiske BL, Kovesdy CP, Nadkarni GN, Shalev V, Segev DL, Coresh J, Lentine KL, Garg AX; for the Chronic Kidney Disease Prognosis Consortium. Kidney-failure risk projection for the living kidney-donor candidate. N Engl J Med 2016;374:411–421. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Tangri N, Grams ME, Levey AS, Coresh J, Appel LJ, Astor BC, Chodick G, Collins AJ, Djurdjev O, Elley CR, Evans M, Garg AX, Hallan SI, Inker LA, Ito S, Jee SH, Kovesdy CP, Kronenberg F, Heerspink HJ, Marks A, Nadkarni GN, Navaneethan SD, Nelson RG, Titze S, Sarnak MJ, Stengel B, Woodward M, Iseki K.. Multinational assessment of accuracy of equations for predicting risk of kidney failure: a meta-analysis. JAMA 2016;315:164–174. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Coresh J, Turin TC, Matsushita K, Sang Y, Ballew SH, Appel LJ, Arima H, Chadban SJ, Cirillo M, Djurdjev O, Green JA, Heine GH, Inker LA, Irie F, Ishani A, Ix JH, Kovesdy CP, Marks A, Ohkubo T, Shalev V, Shankar A, Wen CP, de Jong PE, Iseki K, Stengel B, Gansevoort RT, Levey AS, Prognosis Consortium CKD.. Decline in estimated glomerular filtration rate and subsequent risk of end-stage renal disease and mortality. JAMA 2014;311:2518–2531. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Kovesdy CP, Coresh J, Ballew SH, Woodward M, Levin A, Naimark DM, Nally J, Rothenbacher D, Stengel B, Iseki K, Matsushita K, Levey AS; the CKD Prognosis Consortium. Past decline versus current eGFR and subsequent ESRD risk. J Am Soc Nephrol 2016;27:2447–2455. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Levey AS, Stevens LA, Schmid CH, Zhang YL, Castro AF 3rd, Feldman HI, Kusek JW, Eggers P, Van Lente F, Greene T, Coresh J.. A new equation to estimate glomerular filtration rate. Ann Intern Med 2009;150:604–612. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Levey AS, Coresh J, Greene T, Marsh J, Stevens LA, Kusek JW, Van Lente F.. Expressing the modification of diet in renal disease study equation for estimating glomerular filtration rate with standardized serum creatinine values. Clin Chem 2007;53:766–772. [DOI] [PubMed] [Google Scholar]
- 27. Miller WG, Bruns DE, Hortin GL, Sandberg S, Aakre KM, McQueen MJ, Itoh Y, Lieske JC, Seccombe DW, Jones G, Bunk DM, Curhan GC, Narva AS.. Current issues in measurement and reporting of urinary albumin excretion. Clin Chem 2009;55:24–38. [DOI] [PubMed] [Google Scholar]
- 28. James MT, Grams ME, Woodward M, Elley CR, Green JA, Wheeler DC, de Jong P, Gansevoort RT, Levey AS, Warnock DG, Sarnak MJ, Tonelli M, Hemmelgarn BR, James MT, Turin TC, Coresh J, Matsushita K, Grams M, Sang Y, Shlipak M, Sarnak MJ, Katz R, Wheeler DC, Emberson J, Landray MJ, Townend JN, Green J, Kirchner HL, Perkins R, Chang AR, Romundstad S, Aasarød K, Øien CM, Hallan S, Smith DH, Thorp ML, Johnson ES, Chodick G, Herzel E, Katz R, Shalev V, Gansevoort RT, Bakker SJL, Lambers Heerspink HJ, van der Harst P, Jee SH, Kimm H, Mok Y, Tangri N, Naimark D, Ärnlöv J, Larsson A, Lannfelt L, Kovesdy CP, Kalantar-Zadeh K, Coresh J, Grams M, Matsushita K, Gansevoort RT, de Jong PE, Iseki K, Levey AS, Sarnak MJ, Stengel B, Warnock D, Woodward M, Ballew SH, Coresh J, Grams M, Matsushita K, Sang Y, Woodward M.. A meta-analysis of the association of estimated GFR, albuminuria, diabetes mellitus, and hypertension with acute kidney injury. Am J Kidney Dis 2015;66:602–612. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Hallan SI, Matsushita K, Sang Y, Mahmoodi BK, Black C, Ishani A, Kleefstra N, Naimark D, Roderick P, Tonelli M, Wetzels JF, Astor BC, Gansevoort RT, Levin A, Wen CP, Coresh J.. Age and association of kidney measures with mortality and end-stage renal disease. JAMA 2012;308:2349–2360. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Kovesdy CP. Updates in hyperkalemia: outcomes and therapeutic strategies. Rev Endocr Metab Disord 2017;18:41–47. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Ponikowski P, Voors AA, Anker SD, Bueno H, Cleland JG, Coats AJ, Falk V, Gonzalez-Juanatey JR, Harjola VP, Jankowska EA, Jessup M, Linde C, Nihoyannopoulos P, Parissis JT, Pieske B, Riley JP, Rosano GM, Ruilope LM, Ruschitzka F, Rutten FH, van der Meer P.. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur J Heart Fail 2016;18:891–975. [DOI] [PubMed] [Google Scholar]
- 32. Brenner BM, Cooper ME, de Zeeuw D, Keane WF, Mitch WE, Parving HH, Remuzzi G, Snapinn SM, Zhang Z, Shahinfar S.. Effects of losartan on renal and cardiovascular outcomes in patients with type 2 diabetes and nephropathy. N Engl J Med 2001;345:861–869. [DOI] [PubMed] [Google Scholar]
- 33. Iino Y, Hayashi M, Kawamura T, Shiigai T, Tomino Y, Yamada K, Kitajima T, Ideura T, Koyama A, Sugisaki T, Suzuki H, Umemura S, Kawaguchii Y, Uchida S, Kuwahara M, Yamazaki T; Japanese Losartan Therapy Intended for the Global Renal Protection in Hypertensive Patients Study I . Renoprotective effect of losartan in comparison to amlodipine in patients with chronic kidney disease and hypertension—a report of the Japanese Losartan Therapy Intended for the Global Renal Protection in Hypertensive Patients (JLIGHT) study. Hypertens Res 2004;27:21–30. [DOI] [PubMed] [Google Scholar]
- 34. Lewis EJ, Hunsicker LG, Bain RP, Rohde RD; for the Collaborative Study Group. The effect of angiotensin-converting-enzyme inhibition on diabetic nephropathy. N Engl J Med 1993;329:1456–1462. [DOI] [PubMed] [Google Scholar]
- 35. Maschio G, Alberti D, Janin G, Locatelli F, Mann JF, Motolese M, Ponticelli C, Ritz E, Zucchelli P; the Angiotensin-Converting-Enzyme Inhibition in Progressive Renal Insufficiency Study Group. Effect of the angiotensin-converting-enzyme inhibitor benazepril on the progression of chronic renal insufficiency. N Engl J Med 1996;334:939–945. [DOI] [PubMed] [Google Scholar]
- 36. Randomised placebo-controlled trial of effect of ramipril on decline in glomerular filtration rate and risk of terminal renal failure in proteinuric, non-diabetic nephropathy. The GISEN Group (Gruppo Italiano di Studi Epidemiologici in Nefrologia). Lancet 1997;349:1857–1863. [PubMed] [Google Scholar]
- 37. Hou FF, Zhang X, Zhang GH, Xie D, Chen PY, Zhang WR, Jiang JP, Liang M, Wang GB, Liu ZR, Geng RW.. Efficacy and safety of benazepril for advanced chronic renal insufficiency. N Engl J Med 2006;354:131–140. [DOI] [PubMed] [Google Scholar]
- 38. Bozkurt B, Agoston I, Knowlton AA.. Complications of inappropriate use of spironolactone in heart failure: when an old medicine spirals out of new guidelines. J Am Coll Cardiol 2003;41:211–214. [DOI] [PubMed] [Google Scholar]
- 39. Shah KB, Rao K, Sawyer R, Gottlieb SS.. The adequacy of laboratory monitoring in patients treated with spironolactone for congestive heart failure. J Am Coll Cardiol 2005;46:845–849. [DOI] [PubMed] [Google Scholar]
- 40. Miao Y, Dobre D, Heerspink HJ, Brenner BM, Cooper ME, Parving HH, Shahinfar S, Grobbee D, de Zeeuw D.. Increased serum potassium affects renal outcomes: a post hoc analysis of the Reduction of Endpoints in NIDDM with the Angiotensin II Antagonist Losartan (RENAAL) trial. Diabetologia 2011;54:44–50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Pitt B, Anker SD, Bushinsky DA, Kitzman DW, Zannad F, Huang IZ; on behalf of the PEARL-HF Investigators. Evaluation of the efficacy and safety of RLY5016, a polymeric potassium binder, in a double-blind, placebo-controlled study in patients with chronic heart failure (the PEARL-HF) trial. Eur Heart J 2011;32:820–828. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Buysse JM, Huang IZ, Pitt B.. PEARL-HF: prevention of hyperkalemia in patients with heart failure using a novel polymeric potassium binder, RLY5016. Future Cardiol 2012;8:17–28. [DOI] [PubMed] [Google Scholar]
- 43. Weir MR, Bakris GL, Bushinsky DA, Mayo MR, Garza D, Stasiv Y, Wittes J, Christ-Schmidt H, Berman L, Pitt B; for the OPAL-HK Investigators. Patiromer in patients with kidney disease and hyperkalemia receiving RAAS inhibitors. N Engl J Med 2015;372:211–221. [DOI] [PubMed] [Google Scholar]
- 44. Kosiborod M, Rasmussen HS, Lavin P, Qunibi WY, Spinowitz B, Packham D, Roger SD, Yang A, Lerma E, Singh B.. Effect of sodium zirconium cyclosilicate on potassium lowering for 28 days among outpatients with hyperkalemia: the HARMONIZE randomized clinical trial. JAMA 2014;312:2223–2233. [DOI] [PubMed] [Google Scholar]
- 45. Packham DK, Rasmussen HS, Lavin PT, El-Shahawy MA, Roger SD, Block G, Qunibi W, Pergola P, Singh B.. Sodium zirconium cyclosilicate in hyperkalemia. N Engl J Med 2015;372:222–231. [DOI] [PubMed] [Google Scholar]
- 46. Kovesdy CP. Management of hyperkalemia: an update for the internist. Am J Med 2015;128:1281–1287. [DOI] [PubMed] [Google Scholar]
- 47. Ryden L, Grant PJ, Anker SD, Berne C, Cosentino F, Danchin N, Deaton C, Escaned J, Hammes HP, Huikuri H, Marre M, Marx N, Mellbin L, Ostergren J, Patrono C, Seferovic P, Uva MS, Taskinen MR, Tendera M, Tuomilehto J, Valensi P, Zamorano JL, Zamorano JL, Achenbach S, Baumgartner H, Bax JJ, Bueno H, Dean V, Deaton C, Erol C, Fagard R, Ferrari R, Hasdai D, Hoes AW, Kirchhof P, Knuuti J, Kolh P, Lancellotti P, Linhart A, Nihoyannopoulos P, Piepoli MF, Ponikowski P, Sirnes PA, Tamargo JL, Tendera M, Torbicki A, Wijns W, Windecker S, De BG, Sirnes PA, Ezquerra EA, Avogaro A, Badimon L, Baranova E, Baumgartner H, Betteridge J, Ceriello A, Fagard R, Funck BC, Gulba DC, Hasdai D, Hoes AW, Kjekshus JK, Knuuti J, Kolh P, Lev E, Mueller C, Neyses L, Nilsson PM, Perk J, Ponikowski P, Reiner Z, Sattar N, Schachinger V, Scheen A, Schirmer H, Stromberg A, Sudzhaeva S, Tamargo JL, Viigimaa M, Vlachopoulos C, Xuereb RG.. ESC Guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with the EASD: the Task Force on diabetes, pre-diabetes, and cardiovascular diseases of the European Society of Cardiology (ESC) and developed in collaboration with the European Association for the Study of Diabetes (EASD). Eur Heart J 2013;34:3035–3087. [DOI] [PubMed] [Google Scholar]
- 48. Kovesdy CP, Appel LJ, Grams ME, Gutekunst L, McCullough PA, Palmer BF, Pitt B, Sica DA, Townsend RR.. Potassium homeostasis in health and disease: a scientific workshop cosponsored by the National Kidney Foundation and the American Society Of Hypertension. Am J Kidney Dis 2017;11:783–800. [DOI] [PubMed] [Google Scholar]
- 49. Nakhoul GN, Huang H, Arrigain S, Jolly SE, Schold JD, Nally JV Jr, Navaneethan SD.. Serum potassium, end-stage renal disease and mortality in chronic kidney disease. Am J Nephrol 2015;41:456–463. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50. Heerspink HJ, Gao P, de Zeeuw D, Clase C, Dagenais GR, Sleight P, Lonn E, Teo KT, Yusuf S, Mann JF.. The effect of ramipril and telmisartan on serum potassium and its association with cardiovascular and renal events: results from the ONTARGET trial. Eur J Prev Cardiol 2014;21:299–309. [DOI] [PubMed] [Google Scholar]
- 51. Cremer W, Bock KD.. Symptoms and course of chronic hypokalemic nephropathy in man. Clin Nephrol 1977;7:112–119. [PubMed] [Google Scholar]
- 52. Elger M, Bankir L, Kriz W.. Morphometric analysis of kidney hypertrophy in rats after chronic potassium depletion. Am J Physiol 1992;262:F656–F667. [DOI] [PubMed] [Google Scholar]
- 53. Riemenschneider T, Bohle A.. Morphologic aspects of low-potassium and low-sodium nephropathy. Clin Nephrol 1983;19:271–279. [PubMed] [Google Scholar]
- 54. Torres VE, Young WF Jr., Offord KP, Hattery RR.. Association of hypokalemia, aldosteronism, and renal cysts. N Engl J Med 1990;322:345–351. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.