
Fig. 2.
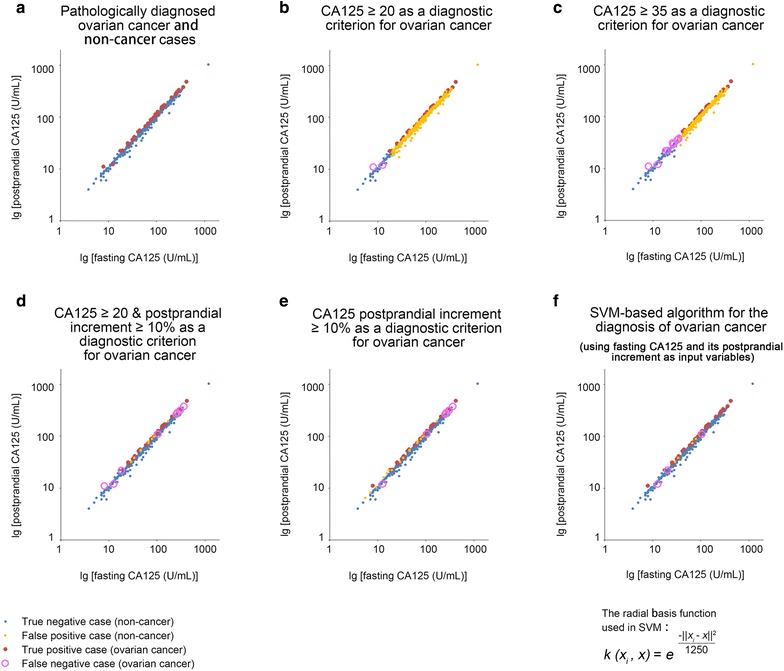
Performances of CA125-based diagnostic criteria in the study population. a The 2-dimensional distribution characteristics of fasting and postprandial CA125 in the enrolled patients. Most of the true positive cases (ovarian cancer cases, red dots) were located at the upper left margin of the scatter diagram, which exhibited higher postprandial increments in CA125 than the true negative cases (non-cancer cases, blue dots). b The diagnostic performance of the CA125 ≥ 20 U/mL criterion. c The diagnostic performance of the CA125 ≥ 35 U/mL criterion. d The diagnostic performance of the CA125 ≥ 20 U/mL plus CA125 increment ≥ 10% criteria. The number of false positive cases (orange dots) was greatly reduced by including an additional CA125 increment ≥ 10% criterion compared with the performance of the CA125 ≥ 20 U/mL criterion alone. e The diagnostic performance of the CA125 increment ≥ 10% criterion. The number of false negative cases (pink circles, 8 cases) was reduced (to 6 cases) by deleting the CA125 ≥ 20 U/mL criterion. f The diagnostic performance of the SVM-based CA125-increment algorithm (the exact form of the RBF kernel function is given). The false positive cases were reduced to 4 cases; and the false negative cases were reduced to 3 cases. The sensitivity (91.7%) and specificity (99.2%) for detecting early-stage ovarian cancer reached their maxima by using this algorithm