
Fig. 3.
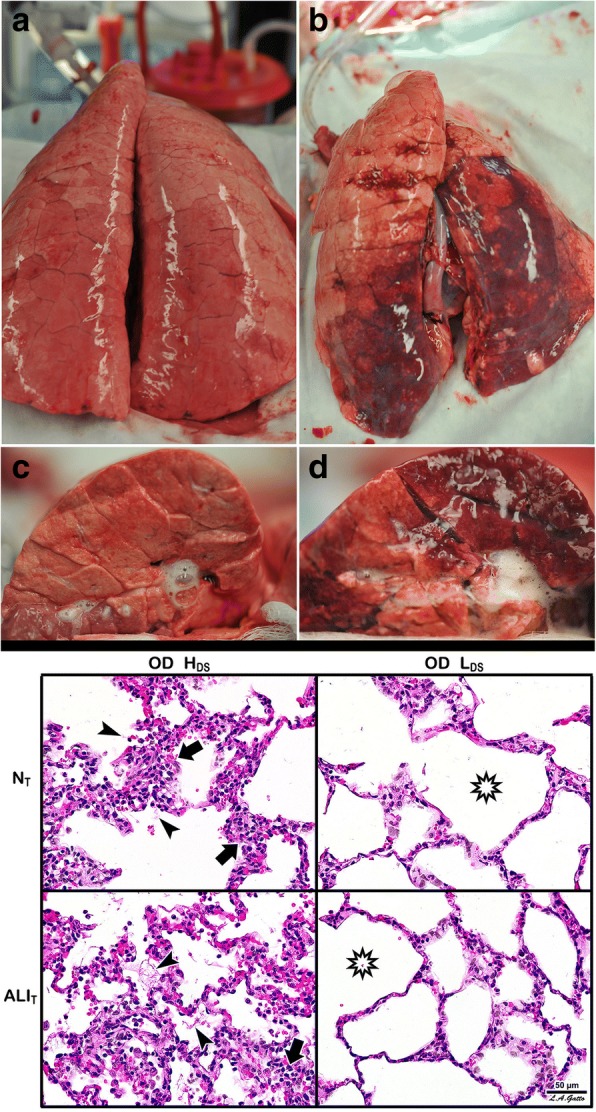
A novel heterogeneous lung injury model in which the impact of any mechanical breath can be tested in both normal (“baby lung”) and the injured (acute respiratory distress syndrome (ARDS)) lung tissues. Heterogeneous injury was caused to very specific areas of lung tissue by instillation of Tween-20 via bronchoscopy into the dependent portion of the diaphragmatic lobe with the pig in the supine position. The remaining lung tissue not exposed to Tween-20 was normal. Following Tween-20 injury animals were split into two groups: either high dynamic strain (HDS) caused by an extended expiratory duration or low dynamic strain (LDS) with a very short expiratory duration. Both groups were exposed to over-distension (plateau airway pressure 40 cmH2O). It is currently believed that high plateau airway pressures (≥ 30 cmH2O) causes ventilator-induced lung injury (VILI) in a heterogeneous ARDS lung by over-distending (OD) the remaining normal tissue (i.e. the baby lung) [34]. The goal of the study was to identify if OD would cause VILI in the baby lung, if OD would exacerbate tissue damage in the Tween-20-injured lung tissue, and if dynamic strain played a role in lung tissue injury and/or protection. Gross Lung Photos: The top panel (a-d) shows the whole lung and the cut lung surface at necropsy. In the OD + LDS group (a, c) the lung was prevented from collapsing at expiration by using a very short expiratory duration. In the OD + HDS group (b, d) the lung was allowed to collapse during expiration by extending the expiratory duration. This study demonstrates that OD did not grossly injure the normal lung tissue, nor did it exacerbate injury in the tissue injured with Tween-20 (a, c), as long as the dynamic strain was minimal. The lung is uniformly inflated (top panel a) and the cut lung surface appears well-inflated without interlobular edema (top panel c). OD combined with HDS (top panel b, d) exacerbated damage in the Tween-20-injured tissue and directly injured the baby lung. The lung showed marked atelectasis, extending into the normal lobes that were not exposed to Tween 20 (top panel b). The cut surface showed extensive atelectasis, interlobular edema (clear jelly-like substance between lobules), and significant airway water and edema foam in the airways (top panel d). This study demonstrates that OD + HDS exacerbated injury to the Tween-20-damaged tissue and caused direct VILI injury to the normal tissue not exposed to Tween 20, whereas OD + LDS caused no injury to the baby lung and did not exacerbate injury in the Tween-20-injured tissue. Lung Histology: The bottom panel shows representative histology staining in both the normal tissue (NT) and the Tween-20-injured lung tissue (ALIT) in both the OD + HDS and OD + LDS groups. OD + HDS caused severe injury to the NT and exacerbated injury in the ALIT tissues. Arrows indicate infiltration of inflammatory white blood cells and the arrowhead identifies the presence of fibrin deposits in the airspace (i.e pulmonary edema). This pathology was not seen in the OD + LDS group and the star shows the improved alveolar patency as compared with the OD + HDS group. This study suggests that OD alone does not injury the baby lung unless combined with high dynamic strain [23]