
Figure 1.
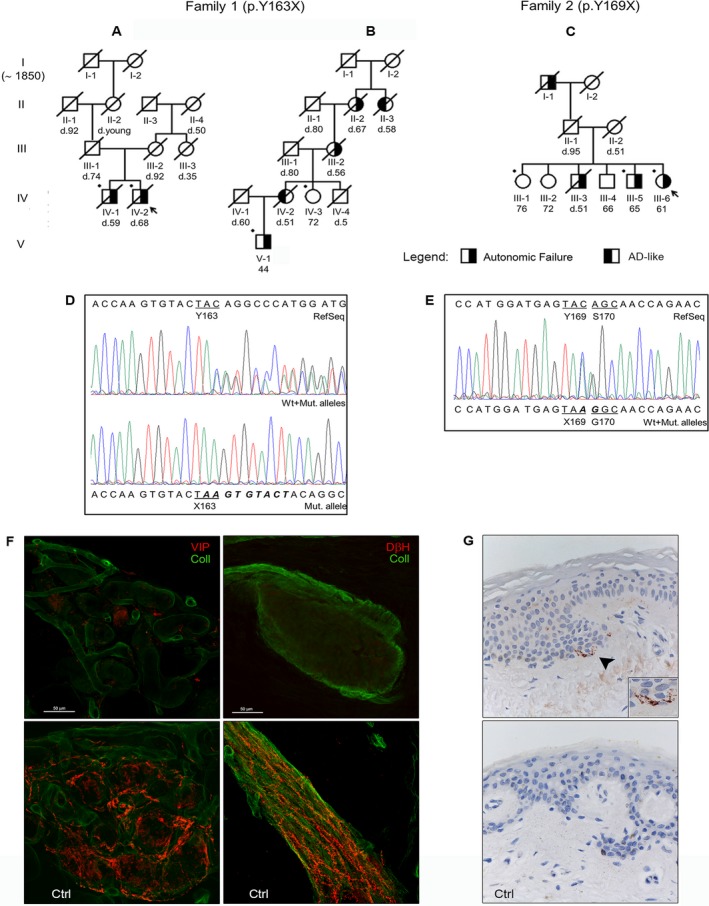
Pedigree of family 1 (A,B) and family 2 (C). Arrows point out the probands, while bullets indicate the subjects who underwent genetic analysis. Although the patient's ancestors of family 1 were traced back to 1850, there was no common founder for family branches A and B; however, the two were likely connected because of the restricted geographical residence area (two cities in adjacent provinces with a cumulative population of ~40,000 people) and the identity of the peculiar genetic mutation. (D and E) Sanger sequencing electropherograms showing the nucleotide sequence surrounding the two mutations (c.478_479insAAGTGTACT resulting in the p.Y163X mutation on the left; c.507C>A determining the p.Y169X mutation on the right). (F) A confocal study (magnification ×400) of autonomic patterns of innervation in the proband 1 (upper boxes) and a control subject. The leg autonomic innervation of sweat gland (left) and arrector pilorum muscle (right) were analyzed. Nerve fibers are marked in red by specific autonomic markers for sweat gland (VIP, vasoactive intestinal peptide) and arrector pilorum muscle (DβH, dopamine‐beta‐hydroxylase), whereas the collagen staining is shown in green. The innervation analysis revealed an almost total loss of cholinergic and noradrenergic fibres in proband 1 compared to the control subject. (G) Immunohistochemical detection of abnormal PrP in proband 1 (upper box) and in a control subject (magnification ×400). PrP staining with primary antibody 3F4 reveals fine, punctate deposits (arrowhead) in the upper dermis at the transition to epidermis only in the patient (the box in the lower‐right corner shows the PrP deposits at a higher magnification).