
Fig. 1. Cumulative incidence rates of VTE.
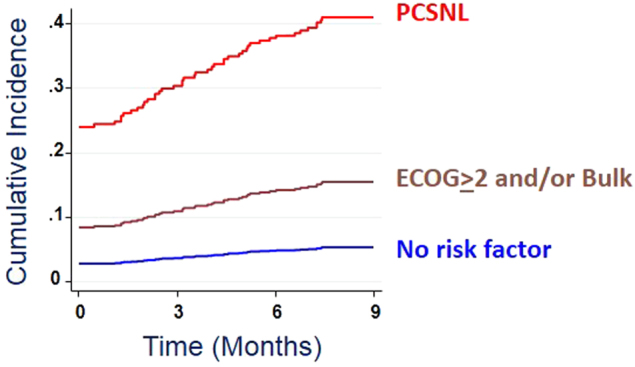
The graph shows the results of a competing risk regression analysis. Death was counted as a competitive event. VTE before the start of systemic therapy were considered heralding events and were counted as events at time 0, while VTE during the first nine months from treatment start was considered treatment-related events. Subdistribution hazard risk was 5.2-fold (95% CI, 3.1–8.8) for patients with the risk factors reduced performance status (ECOG > 2) and/or bulky disease (>10 cm), and 8.0-fold (95% C.I., 3.7–17.5) for patients with PCNSL.Analysis of the treatment-related VTE in 803 patients, after exclusion of the 54 ones who presented with VTE before the start of therapy, confirmed a VTE risk gradient similar to that of the overall cohort (see text) (5/29, 17.2% in PCNSL, 25/333, 7.5% in the bulk and/or ECOG group, and 11/441, 2.5% in the low-risk group)