

Abstract
Congenital anomalies of tongue are rare disorders usually associated with syndromes. In present article we describe a case of a non-syndromic adult patient with bifid tongue with salivary hamartoma on the dorsum of the tongue. We described the clinical features, problems faced by the patient and management. As etiology is uncertain we should have proper understanding of embryology.
Keywords: Bifid tongue, nonsyndromic, salivary hamartoma
INTRODUCTION
Bifid tongue is a rare congenital malformation usually associated with syndromes such as orofacial digital syndrome and facial clefts.[1] The cleft may be seen dividing the tongue at the midline or laterally with complete or partial separation. Congenital bifid tongue occurs due to disturbances in the fusion of the median and two lingual swellings during intrauterine life.[2] Congenital bifid tongue is reported to occur with associated tissue growth that mostly constitutes hamartomas. They are usually diagnosed and surgically corrected early in life. The clinical presentation and its influence in a nonsyndromic adult have not been previously reported. Herein, we describe the clinical features and the surgical outcome of a nonsyndromic young man who was diagnosed with a salivary hamartoma associated with a bifid tongue.
CASE REPORT
A 22-year-old Sinhalese male patient presented to our clinic with a complaint of difficulty in swallowing and speaking due to a large growth on the dorsum of his tongue. It had been present from birth and had gradually enlarged over time. Due to the prevailing civil war in the country for over 30 years, he has had limited access to an Oral and Maxillofacial Surgery care during the past years and had been forced to live with this deformity. Though painless, the swelling affected his speech as his articulation was altered. In addition, the lump on his tongue caused difficulty in forming a food bolus and swallowing it, while the bifid tongue affected the cleansing of his mouth. The appearance of the abnormal shape of his tongue had harshly influenced his social life and he was subjected to bullying. He was nonsyndromic, and no other congenital anomalies were detected. On local examination, an asymmetrically bifid tongue involving the left side was noted. A large, firm, pink, nontender tissue mass was seen at the center of the tongue [Figure 1].
Figure 1.

Benign tumor on the dorsum of tongue and the bifid tongue is seen on the left side
A lingual thyroid was suspected initially, but the iodine scan showed normal functioning of the thyroid tissue in the anterior neck. Interestingly, iodine was noted to collect in the tongue mass as well, and thereby suggesting salivary/thyroid origin. The patient was otherwise healthy. The treatment plan was the complete removal of the growth and correction of the bifid tongue by closing the primary (or primarily closing it) under general anesthesia [Figure 2]. No intraoperative complications were encountered, and full function of the tongue was preserved. The excised growth was sent for histopathological examination. Two weeks later, the patient was followed up in the speech clinic to assist in speech and swallowing. The histopathology reported that the mass was predominantly mucous salivary tissue. It showed both mixed and mucous lobules, and the histological diagnosis was a salivary hamartoma. The patient had no recurrences at 1-year follow-up.
Figure 2.
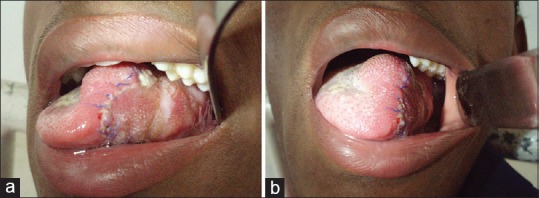
(a) Postoperative image after removal of salivary hamartoma and correction of bifid tongue in lateral view. (b) frontal view
DISCUSSION
The anterior two-thirds of the tongue is formed through the fusion of two lateral lingual tubercles which arise from the pharyngeal arches. Developmental malformations of the tongue can be classified as major or minor, or single or multiple. Microglossia, hemiatrophy, aglossia, hemihypertrophy, macroglossia, cleft/bifid tongue, long tongue, ankyloglossia, hamartomatous lesions, and lingual thyroids are some congenital anomalies reported to be associated with the tongue.[3] Bifid tongue is generally associated with various syndromes.[4] This case was not associated with any other developmental abnormalities, and thus, it was considered as a nonsyndromic condition. In 1945, Stamm and Tauber for the first time reported a lingual hamartoma which contained adipose tissue, mucosal glands muscle fibers, and fibrous tissue.[5] Since 1985, only 16 cases of bifid tongues in nonsyndromic patients have been reported in literature. Out of 16 cases, only 3 cases were salivary hamartomas.[6,7,8] A benign salivary hamartoma may cause hypoplasia of the tongue and lead to the formation of a bifid tongue. However, the origin of salivary hamartoma is uncertain. It is hypothesized that a developmental malformation of the salivary gland which may occur at the 3rd embryonal week may result in a lateral lingual tubercle which can disturb the process of fusion and result in the division of the tongue.[8] As these benign lesions increases in size, it may cause several functional problems such as positional dyspnea, difficulty in swallowing, cyanosis, bradycardia, and interference in speech.[9] In our patient, difficulty in swallowing and interference in speech were completely resolved after surgery and speech therapy.
CONCLUSION
Abnormalities such as bifid tongue and hamartomas should be diagnosed and treated in early life. In case of an adult presentation, surgery and rehabilitation treatment restore normal function of the tongue.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Gurrieri F, Franco B, Toriello H, Neri G. Oral-facial-digital syndromes: Review and diagnostic guidelines. Am J Med Genet A. 2007;143A:3314–23. doi: 10.1002/ajmg.a.32032. [DOI] [PubMed] [Google Scholar]
- 2.Takagia Y, Machidaab J, Satoa H, Sakumaa, Nodaa H, Oh-iwaa I. Congenital bifid tongue with lingual hamartoma: A case report and review of the literature. J Oral Maxillofac Surg Med Pathol. 2016;28:133–7. [Google Scholar]
- 3.Emmanouil-Nikoloussi E, Kerameos-Foroglou C. Congenital syndromes connected with tongue malformations. Bull Assoc Anat (Nancy) 1992;76:67–72. [PubMed] [Google Scholar]
- 4.Albrecht H. Uber hamartoma. Verh Dtsch Pathol Ges. 1904;7:153. [Google Scholar]
- 5.Stamm C, Tauber R. Hamartoma of the tongue. Laryngoscope. 1945;55:140. [Google Scholar]
- 6.Surej KL, Kurien NM, Sivan MP. Isolated congenital bifid tongue. Natl J Maxillofac Surg. 2010;1:187–9. doi: 10.4103/0975-5950.79228. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Shi J, Zhang J, Ding M, Cao Q. Lower lip cleft, bifid tongue and fibrolipoma: A case report of rare congenital anomaly. Br J Oral Maxillofac Surg. 2014;52:e36–8. doi: 10.1016/j.bjoms.2014.04.003. [DOI] [PubMed] [Google Scholar]
- 8.Miyamoto Y, Nagayama M, Hayashi Y. A cleft palate child with lobulated tongue and lingual hamartoma: Report of a case. J Oral Maxillofac Surg. 1991;49:644–6. doi: 10.1016/0278-2391(91)90348-p. [DOI] [PubMed] [Google Scholar]
- 9.Bhattacharya V, Khanna S, Bashir SA, Kumar U, Garbyal RS. Cleft palate associated with hamartomatous bifid tongue. Report of two cases. J Plast Reconstr Aesthet Surg. 2009;62:1442–5. doi: 10.1016/j.bjps.2008.01.034. [DOI] [PubMed] [Google Scholar]