
Fig. 2. How tumor genotypes and phenotypes shape the TIME.
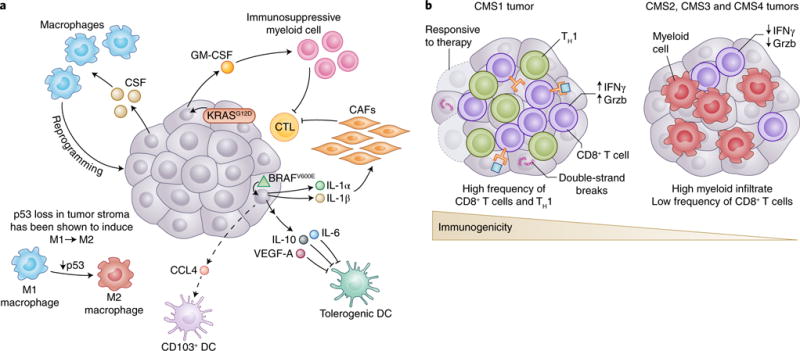
a, Tumors are known to establish protumoral and immunosuppressive environments to support their growth and promote immune evasion. Central to building an immunosuppressive TIME are oncogenes and aberrant signaling pathways that lead to the production of cytokines and chemokines with potent effects. The tumor shown is representative of a spectrum of cancer types. In melanoma, BRAFV600E (green triangle) has been shown to induce constitutive WNT/β-catenin signaling, which in turn decreases production of CCL4, a chemokine important for the recruitment of CD103+ DCs. Additionally, BRAFV600E has been shown to induce expression of factors such as IL-10 and IL-1α, which can induce tolerogenic forms of DC and cancer-associated fibroblasts (CAFs), respectively. Oncogenic KRASG12D in PDAC leads to the secretion of GM-CSF, corresponding to increased development of CD11b+ myeloid cells with reported immunosuppressive function. Deficiency in p53 in hepatic stellate cells, a stromal population, leads to production of factors that polarize TAMs from the immunoactivating M1 phenotype to the immunosuppressive M2 phenotype. Interestingly, many tumors have been shown to secrete high levels of the monocyte/macrophage-promoting cytokine CSF-1. b, The mutational landscape of tumors can profoundly affect the quality and character of the TIME. In CRC, there are four consensus molecular subtypes (CMS1-4). CMS1 is defined by defects in DNA mismatch repair leading to microsatellite instability or hypermutation rates. Because of the abundance of possible neoepitopes, CTL infiltration is generally high, and CTLs display gene expression patterns indicative of an ongoing immune response. Patients with CMS1 tumors have generally more favorable outcomes with checkpoint-blockade treatment than do patients with CMS2-4. Although there are differences in the histological and immunological character of CMS2, 3 and 4 CRC subtypes, they are generally less immune infiltrated, as is suggestive of antigenically cold tumors.