
Fig. 2. Lymph node metastatic cancer cells can colonize the lung.
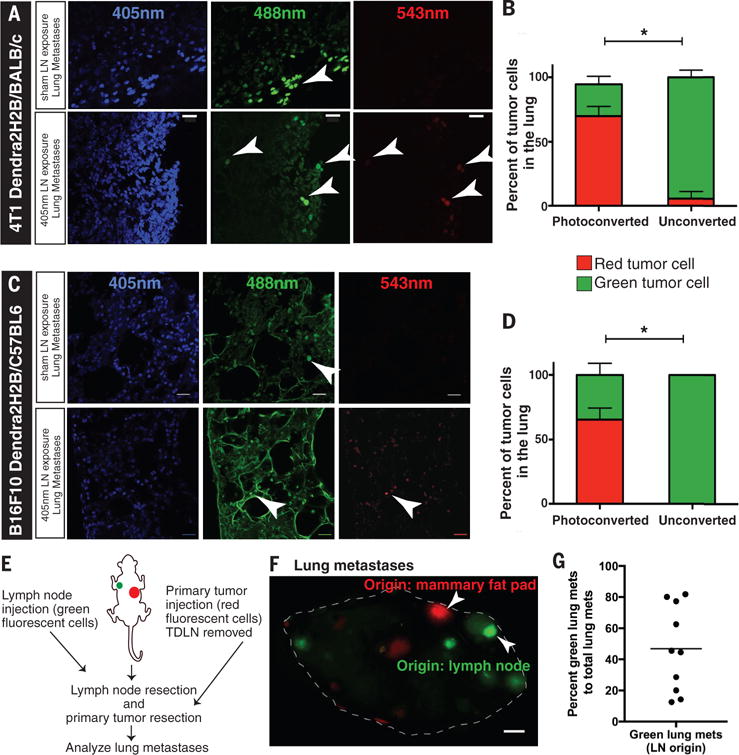
(A, C) 100μm sections of fresh frozen lungs were obtained from Dendra2H2B-4T1 and Dendra2H2B-B16F10 tumor-bearing mice that either had their lymph node photoconverted with a 405nm diode or had no photoconversion. The top panels are representative images of micrometastatic disease (arrowheads) in the lung from control animals (no photoconversion), whereas the bottom panels show photoconverted isolated cancer cells that have colonized the lung via the lymph node. Scale bar=20μm. (B, D) The percentage of cancer cells detected in the lungs of Dendra2H2B-4T1 (n=8) and Dendra2H2B-B16F10 (n=8) tumor-bearing mice that were green (not photoconverted) versus red (photoconverted cells) are shown. *p<0.05 comparing 405nm light exposure (Photoconverted) to sham light exposure (Unconverted) for individual cells lines. (E) Schematic of experiment to determine whether cancer cells injected directly in the lymph node and in the mammary fat pad (MFP) can both form large metastases in the lungs. (F) Image of a lung with red lesions (originating from MFP) and green lesions (originating from lymph node) marked by arrowheads. Scale bar=1mm. (G) Lung metastases are represented as a percentage of lymph node origin metastasis (green) to total macroscopic lesions (red + green) (n=10). Using a one-sample Student’s t-test, both lymph node and MFP origin tumors had an incidence greater than zero (p<0.001).